
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

0.4
Cite Score
SJR: 0.114 / SNIP: 0.090
Volume 13, Issue 2 (2021)
Iran J War Public Health 2021, 13(2): 97-102 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2021/05/16 | Accepted: 2021/08/2 | Published: 2021/09/22
Received: 2021/05/16 | Accepted: 2021/08/2 | Published: 2021/09/22
How to cite this article
Azarmi S, Zareiyan A, Baniyaghoobi F, Farsi Z, Safshekan S. Psychometric Properties of Roy's Adaptation Questionnaire on Veterans with Lower Limb Amputation. Iran J War Public Health 2021; 13 (2) :97-102
URL: http://ijwph.ir/article-1-975-en.html
URL: http://ijwph.ir/article-1-975-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Department of Health in Disasters and Emergencies, Faculty of Nursing, Aja University of Medical Sciences, Tehran, Iran
2- Public Health Department, Faculty of Nursing, Aja University of Medical Sciences, Tehran, Iran
3- Department of Military Nursing, Faculty of Nursing, Aja University of Medical Sciences, Tehran, Iran
4- Research and Community Health Departments, Faculty of Nursing, Aja University of Medical Sciences, Tehran, Iran
5- Janbazan Medical and Engineering Research Center (JMERC), Tehran, Iran
2- Public Health Department, Faculty of Nursing, Aja University of Medical Sciences, Tehran, Iran
3- Department of Military Nursing, Faculty of Nursing, Aja University of Medical Sciences, Tehran, Iran
4- Research and Community Health Departments, Faculty of Nursing, Aja University of Medical Sciences, Tehran, Iran
5- Janbazan Medical and Engineering Research Center (JMERC), Tehran, Iran
Full-Text (HTML) (1279 Views)
Introduction
War has direct and indirect effects on soldiers' physical and mental health, veterans, and victims [1]. According to the statistics of the Veterans Foundation, more than 400,000 veterans (with spinal, chemical, psychological, and amputation problems) are living in the country [2]. About 20,801 people in Iran suffered from upper or lower limb amputations caused by the Iran-Iraq War in 1980-1988, of which approximately 12,981 patients had lower extremity amputations at various levels [3]. Any defect in the organs of the body can affect different aspects of human life [4]. Amputation is one of the most disturbing events that people may experience in their life [5]. In countries that have recently experienced war, about 80% have experienced amputations [6].
The most common amputation due to war injuries is lower limb amputation [7]. Amputation causes a severe decrease in physical activity and mobility of the persons and prevents them from performing their natural role, and leads to significant problems in their lives [8]. Therefore, it is necessary to take interventions to make a normal life and compatibility with the created conditions for these patients [9]. However, the passage of time increases the adaptation of chronic patients to their disease. Because resilience is a dynamic process, and people can adapt to the situation over time. This process allows them to maintain their healthy function [10].
Evidence has shown that in chronic diseases, patients' adaptation to long-term side effects has an effective role in controlling the disease and improving their quality of life [4, 9, 11]. One of the practical and effective models in nursing is the Roy Adaptation Model [12, 13]. Roy considers the degree of adaptation as the effects of the three principal, contextual and residual stimuli. Manipulation of these stimuli during the care program increases the rate of adaptation and thus better control of the disease. It also states that adaptation includes physical adaptation (physiological dimension) and psychological adaptation (self-perception, role-playing, independence/dependence) [14].
The results of several studies showed an improvement in caring activities, concentration, organization of care for chronic patients, and an increase in adaptive responses in these patients in all four dimensions of the Roy Adaptation Model, after interventions based on this model [11-15, 17]. The results of other studies showed that guided training based on the Roy Adaptation Model improves adaptation and coping strategies in veterans with lower-limb amputation [4, 9].
Veterans with lower limb amputation have suffered from this condition for many years. Therefore, assessing their compatibility to perform physical, mental, and social health interventions requires access to a standard instrument. Researchers designed the Roy Adaptation Questionnaire in veterans with limb amputation and confirmed its face validity, content validity index (CVI), and content validity ratio (CVR). However, the psychometrics of this tool has not been performed yet. Therefore, due to the high number of veterans with lower limb amputation, especially in Iran, and the need to assess and improve their compatibility, the present study aimed to psychoanalyze the Roy Adaptation Questionnaire in veterans with lower limb amputation.
Instrument and Methods
This descriptive study was carried out on 325 veterans with lower limb amputation referred to the Veterans Clinic of the Kosar Orthosis and Prosthesis Center in Tehran in 2018. Four hundred fifty veterans with lower extremity amputation were included in the study by convenience sampling method. The sample size was determined following the necessary standards to apply the factor analysis method. The acceptable sample size for factor analysis is proportional to the number of tool items, and 5-10 people were considered for each item [19].
Three hundred veterans with lower extremity amputation were studied to assess factor validity (exploratory factor analysis) according to the rule of thumb for determining the sample size in factor analysis and the number of items of the instrument (in various studies, the sample size of 300 people has been considered suitable for exploratory factor analysis [20]). Participants were selected and studied with maximum diversity. The inclusion criteria were the ability to read and write, a range of age lower than 65, and a lack of a psychological, spinal cord, and chemical injury. The exclusion criteria as unwillingness to continue participating in the study. The demographic questionnaire was used to investigate the education occupation and marital status. The initial version of the Roy compatibility pattern questionnaire [18] was used through a review of research and resources in the ROV compatibility pattern and its four dimensions, and the extraction of the concept of compatibility based on this model and its main dimensions for veterans with lower limb amputation. Based on previous results, content validity ratio (CVR) and content validity index (CVI) including 35 questions in four physiological (15 items), self-concept (11 items), dependence/independence (4 items) and role-play (5 items) were more than 0.51 and 0.79, respectively [18]. The scoring of the items is based on the 5-points Likert scale (never, rarely, sometimes, most of the time, and always). The scoring is based on mathematical logic [22], ranging from a minimum score of 20 to 100. The higher scores show the higher compatibility in the subjects. Items 1, 4, 5, 6, 7, and 8 in the physiological dimension and items 1 and 2 in the dependence/independence dimension were scored reversely. The scores of 36-20, 52-36, 68-52, 84-68, and 100-84 represent very weak, poor, moderate, good, and very good compatibility. The moral principles raised in the Declaration of Helsinki were respected [21].
The ethical principles of this research are receiving approval of the Engineering and Medical Research Institute of Veterans, oral consent from the subjects studied, observance the principle of confidential information, freedom of participants for canceling their participation at any time of the research, observance the rights of the authors in using texts and electronic resources. The questionnaires were provided to the Veterans Clinic of the Kosar Orthosis and Prosthesis Center subjects by one researcher who received the necessary training. KMO (Kaser-Meyer-Olkin) method was used to confirm factor validity. The factor analysis method is one of the most reliable methods in determining the structures of instruments that measure the psychological characteristics, and the researcher can ensure the validity of their tools for the target population using this method. KMO was calculated, and a Bartlett test was used to evaluate the adequacy of sampling. To determine the reliability of the instruments by the test-retest method and reporting the Intra Class Correlation, 25 veterans with lower limb amputation filled out the questionnaires twice at an interval of 2 weeks; also, the internal adaptation of the instrument was evaluated using Cronbach's alpha test through SPSS 22 software.
Findings
Three hundred twenty-five veterans participated in the study. The average age of the subjects was 53.85±4.63. The demographic characteristics of the subjects are shown in Table 1.
Table 1) Frequency of demographic characteristics of the subjects (N=300)

The rate of KMO ratio was higher than 7.0; therefore, the data had the necessary adequacy for exploratory factor analysis. There was a sufficient correlation between the items based on Bartlett's sphericity test (Table 2). 4 factors were extracted according to the scree plot (Chart 1).
The results showed four factors with an explanation of 47.578% of variances. The factor load of each variable for each of the factors was calculated separately (Table 3). In this matrix, the variables with a high correlation with each other were assigned within a factor. The factor loads were between 0.40-0.76, which were more than 0.3, and showed significance levels.
Table 2) Results of the KMO sampling index and Bartlett's sphericity test
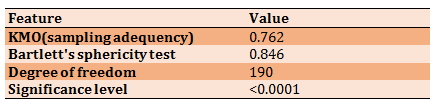

Chart 1) Number of factors of Roy Adaptation Questionnaire on veterans with lower limb amputation
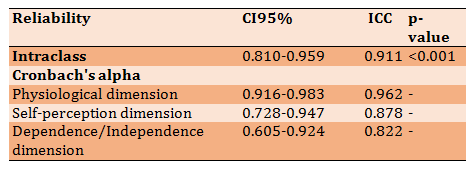
Some of the items that were considered in the dimensions in the initial questionnaire were transferred to other dimensions based on the results of the factor load, due to more consistency with the studied and influential areas in other dimensions or because the participants did not think enough in response to the questionnaire items. Accordingly, the first question in the "dependence/independence" dimension has transferred to the seld-perception dimension. Also, according to the factor analysis results, the number 7 question has transferred to the "dependence/independence" dimension. Also, according to the factor analysis results, out of 35, 7, 5, 1, and 2 items of the physiologic, self-perception, dependence-independence, and role-playing were removed, respectively, due to the lack of factor load in any of the factors. Therefore, the number of items in the questionnaire was reduced from 35 to 20 items. Finally, the questionnaires were filled out by 25 subjects. The reliability results of the questionnaire are shown in Table 4.
War has direct and indirect effects on soldiers' physical and mental health, veterans, and victims [1]. According to the statistics of the Veterans Foundation, more than 400,000 veterans (with spinal, chemical, psychological, and amputation problems) are living in the country [2]. About 20,801 people in Iran suffered from upper or lower limb amputations caused by the Iran-Iraq War in 1980-1988, of which approximately 12,981 patients had lower extremity amputations at various levels [3]. Any defect in the organs of the body can affect different aspects of human life [4]. Amputation is one of the most disturbing events that people may experience in their life [5]. In countries that have recently experienced war, about 80% have experienced amputations [6].
The most common amputation due to war injuries is lower limb amputation [7]. Amputation causes a severe decrease in physical activity and mobility of the persons and prevents them from performing their natural role, and leads to significant problems in their lives [8]. Therefore, it is necessary to take interventions to make a normal life and compatibility with the created conditions for these patients [9]. However, the passage of time increases the adaptation of chronic patients to their disease. Because resilience is a dynamic process, and people can adapt to the situation over time. This process allows them to maintain their healthy function [10].
Evidence has shown that in chronic diseases, patients' adaptation to long-term side effects has an effective role in controlling the disease and improving their quality of life [4, 9, 11]. One of the practical and effective models in nursing is the Roy Adaptation Model [12, 13]. Roy considers the degree of adaptation as the effects of the three principal, contextual and residual stimuli. Manipulation of these stimuli during the care program increases the rate of adaptation and thus better control of the disease. It also states that adaptation includes physical adaptation (physiological dimension) and psychological adaptation (self-perception, role-playing, independence/dependence) [14].
The results of several studies showed an improvement in caring activities, concentration, organization of care for chronic patients, and an increase in adaptive responses in these patients in all four dimensions of the Roy Adaptation Model, after interventions based on this model [11-15, 17]. The results of other studies showed that guided training based on the Roy Adaptation Model improves adaptation and coping strategies in veterans with lower-limb amputation [4, 9].
Veterans with lower limb amputation have suffered from this condition for many years. Therefore, assessing their compatibility to perform physical, mental, and social health interventions requires access to a standard instrument. Researchers designed the Roy Adaptation Questionnaire in veterans with limb amputation and confirmed its face validity, content validity index (CVI), and content validity ratio (CVR). However, the psychometrics of this tool has not been performed yet. Therefore, due to the high number of veterans with lower limb amputation, especially in Iran, and the need to assess and improve their compatibility, the present study aimed to psychoanalyze the Roy Adaptation Questionnaire in veterans with lower limb amputation.
Instrument and Methods
This descriptive study was carried out on 325 veterans with lower limb amputation referred to the Veterans Clinic of the Kosar Orthosis and Prosthesis Center in Tehran in 2018. Four hundred fifty veterans with lower extremity amputation were included in the study by convenience sampling method. The sample size was determined following the necessary standards to apply the factor analysis method. The acceptable sample size for factor analysis is proportional to the number of tool items, and 5-10 people were considered for each item [19].
Three hundred veterans with lower extremity amputation were studied to assess factor validity (exploratory factor analysis) according to the rule of thumb for determining the sample size in factor analysis and the number of items of the instrument (in various studies, the sample size of 300 people has been considered suitable for exploratory factor analysis [20]). Participants were selected and studied with maximum diversity. The inclusion criteria were the ability to read and write, a range of age lower than 65, and a lack of a psychological, spinal cord, and chemical injury. The exclusion criteria as unwillingness to continue participating in the study. The demographic questionnaire was used to investigate the education occupation and marital status. The initial version of the Roy compatibility pattern questionnaire [18] was used through a review of research and resources in the ROV compatibility pattern and its four dimensions, and the extraction of the concept of compatibility based on this model and its main dimensions for veterans with lower limb amputation. Based on previous results, content validity ratio (CVR) and content validity index (CVI) including 35 questions in four physiological (15 items), self-concept (11 items), dependence/independence (4 items) and role-play (5 items) were more than 0.51 and 0.79, respectively [18]. The scoring of the items is based on the 5-points Likert scale (never, rarely, sometimes, most of the time, and always). The scoring is based on mathematical logic [22], ranging from a minimum score of 20 to 100. The higher scores show the higher compatibility in the subjects. Items 1, 4, 5, 6, 7, and 8 in the physiological dimension and items 1 and 2 in the dependence/independence dimension were scored reversely. The scores of 36-20, 52-36, 68-52, 84-68, and 100-84 represent very weak, poor, moderate, good, and very good compatibility. The moral principles raised in the Declaration of Helsinki were respected [21].
The ethical principles of this research are receiving approval of the Engineering and Medical Research Institute of Veterans, oral consent from the subjects studied, observance the principle of confidential information, freedom of participants for canceling their participation at any time of the research, observance the rights of the authors in using texts and electronic resources. The questionnaires were provided to the Veterans Clinic of the Kosar Orthosis and Prosthesis Center subjects by one researcher who received the necessary training. KMO (Kaser-Meyer-Olkin) method was used to confirm factor validity. The factor analysis method is one of the most reliable methods in determining the structures of instruments that measure the psychological characteristics, and the researcher can ensure the validity of their tools for the target population using this method. KMO was calculated, and a Bartlett test was used to evaluate the adequacy of sampling. To determine the reliability of the instruments by the test-retest method and reporting the Intra Class Correlation, 25 veterans with lower limb amputation filled out the questionnaires twice at an interval of 2 weeks; also, the internal adaptation of the instrument was evaluated using Cronbach's alpha test through SPSS 22 software.
Findings
Three hundred twenty-five veterans participated in the study. The average age of the subjects was 53.85±4.63. The demographic characteristics of the subjects are shown in Table 1.
Table 1) Frequency of demographic characteristics of the subjects (N=300)
The rate of KMO ratio was higher than 7.0; therefore, the data had the necessary adequacy for exploratory factor analysis. There was a sufficient correlation between the items based on Bartlett's sphericity test (Table 2). 4 factors were extracted according to the scree plot (Chart 1).
The results showed four factors with an explanation of 47.578% of variances. The factor load of each variable for each of the factors was calculated separately (Table 3). In this matrix, the variables with a high correlation with each other were assigned within a factor. The factor loads were between 0.40-0.76, which were more than 0.3, and showed significance levels.
Table 2) Results of the KMO sampling index and Bartlett's sphericity test
Chart 1) Number of factors of Roy Adaptation Questionnaire on veterans with lower limb amputation
Some of the items that were considered in the dimensions in the initial questionnaire were transferred to other dimensions based on the results of the factor load, due to more consistency with the studied and influential areas in other dimensions or because the participants did not think enough in response to the questionnaire items. Accordingly, the first question in the "dependence/independence" dimension has transferred to the seld-perception dimension. Also, according to the factor analysis results, the number 7 question has transferred to the "dependence/independence" dimension. Also, according to the factor analysis results, out of 35, 7, 5, 1, and 2 items of the physiologic, self-perception, dependence-independence, and role-playing were removed, respectively, due to the lack of factor load in any of the factors. Therefore, the number of items in the questionnaire was reduced from 35 to 20 items. Finally, the questionnaires were filled out by 25 subjects. The reliability results of the questionnaire are shown in Table 4.
Table 3) Factors extracted from factor analysis using Promax rotation and structure matrix of items

Table 4) Results of intraclass reliability and Cronbach's alpha by factors (n=25)
Discussion
Due to the lack of standard questionnaires to assess adaptation based on the Roy model in veterans with lower limb amputation, the present study aimed to psychometrics of the instrument.
Amputated veterans have problems adapting to their "physiological" dimension due to their chronic illness's physical and psychological effects. According to the Roy Adaptation Model and studies in this field, the questionnaire items in the physiological dimension include five basic physiological needs, including activity and rest, nutrition, defecation, oxygenation, and protection [23]. In the dimension of "self-perception", Roy introduces three cases of self-objectivity, self-personality, and self concerning others [24]. The findings also indicate the importance of personality and psychological characteristics of amputated veterans, self-satisfaction and activities, and interaction with family and community in the dimension of "self-perception". According to Roy, the problems that need to be considered in the "role play" dimension are as follows: 1) Role-playing failure in which a person is unable to perform previous behaviors about her/his role; 2) Role conflict when others' expectations of the individual differ from one's own [24]. The questionnaire items designed in the role-playing dimension also showed the problems of veterans in this dimension; because veterans, depending on their physical and mental condition may have conflicts or inadequacies in the roles and abilities of themselves and others. The "independence/dependency" dimension focuses on how people communicate, their goals, structure, and the extent of their relationships [25]. Problems with this dimension can occur in the following two ways: 1) disorder in being dependent; 2) disorder in being independent. Problems in this dimension may also arise in rejection, aggression, violence, competition, lack of cooperation, and desire to be alone [23]. The items related to this dimension of the questionnaire also focus on the communication and support system veterans.
Based on the research background, it was found that several studies have been performed to evaluate the adaptation based on the Roy Adaptation Pattern in different target groups; in each of these studies, a tool has been used to evaluate and measure the compatibility of patients. In the Kisacık study, investigating nursing interventions based on the Roy adaptation pattern in patients undergoing hemiglossectomy surgery, behaviors of the patients were assessed in four dimensions of Roy adaptation pattern, and objective and subjective information was recorded [26]. This study is consistent with the present study in terms of examining the four dimensions of the Roy model; however, due to the difference in observational behavior and results of the interventions and the research community, it is not consistent with our study. In a study, Kavradim investigated the effect of intervention based on the Roy Adaptation Model by training and telephone follow-up method on the quality of self-efficacy of patients after myocardial infarction. In this study, the Roy Adaptation Scale developed by Calista Roy was used to evaluate the adaptation process [27]. In another study, an instrument was designed to investigate the effect of an educational program based on the Roy Adaptation Model on the adaptation of patients with obstructive pulmonary disease. Like the previous study instrument, it included all the dimensions of the Roy adaptation model. However, the instrument psychometrics was not assessed [15]. Lee et al. used the Roy adaptation model in developing prenatal screening tools [28]. In the designed instrument of Lee et al., all four dimensions of the Roy Adaptation Model have been considered, and the psychometrics of the instrument has been assessed, but their research is different from the present research in terms of the statistical population. In another study performed on diabetic patients, the instrument used was the Roy recognition and recognition form, in which the physiological dimension of the samples was not assessed due to the specific conditions of diabetic patients. Using this form, patients were interviewed [29]. In addition to reviewing the Roy Adaptation Pattern in all four dimensions and performing instrument psychometrics, the instrument is designed to be easier to analyze and requires less time.
Mohammadpour investigated the effect of intervention based on the Roy Adaptation Model on self-perception in first pregnant women. The research instrument was a questionnaire to assess the level of adaptation in the dimension of self-perception based on the Roy Adaptation Model consisting of three areas of "spiritual-moral self, self-stability and expected self" and a total of 22 items ranked on the Likert scale. The instrument of the above study includes only one dimension of the Roy Adaptation Model, and, unlike the present study, the psychometrics of the instrument has not been measured, and the research community is different. Various other studies were conducted to investigate the effect of implementing a care program based on the Roy Adaptation Model on different research units [31-33]. In the mentioned studies, as in the present study, all four dimensions of the Roy Adaptation Model were examined, but these studies are not in accordance with the present study in terms of the research community and the lack of instrument psychometrics. In another study that examined the effect of a care program on the physiological adaptation of type 2 diabetic patients based on the Roy Adaptation Model, the instrument included the descriptive items of Roy's four dimensions [11]. It is difficult to fill out the descriptive questionnaires by patients and nurses, and its analysis requires more time. Therefore, the researchers found it necessary to design an instrument that is easier to analyze and requires less time. So, Hekary, in a study on women with coronary artery disease, used various scales to assess four dimensions of the Roy Adaptation Model [17].
In addition to designing the items based on the Roy Adaptation Model, attempts have been made to address all subscales related to the four dimensions based on the framework of this model, and psychometrics of this model has been performed, which is effective in designing the proper instrument. Efforts were also made to design the objective and behavioral items so that veterans with lower-limb amputations could easily understand and answer them. It is recommended to conduct more research to use this instrument more comprehensively in different clinical centers for veterans and to conduct similar research to design similar instruments for different target groups. Health care professionals, especially nurses, can use this instrument in clinical centers to provide more effective care to veterans with lower limb amputation and take effective steps to improve these patients' adaptation and quality of life.
In such studies, a cumulative variance probability of less than 50% is not unexpected; because the samples may not have the right conditions to respond, and the sample size is limited, which is one of the research limitations.
Conclusion
The designed instrument has the face, content, factor validities, and acceptable reliability, which indicate its suitability for measuring the compatibility of veterans with lower limb amputation based on the Roy Adaptation Model and providing better services in the field of care for these patients.
Acknowledgments: The authors appreciated the participation and cooperation of the officials of the Janbazan Medical and Engineering Research Center, management of Kosar Orthosis and Prosthesis Center, veterans clinics affiliated with this center, and the veterans participating in this research.
Ethical Permissions: This article is retrieved from the research project approved by the ethics committee of the Janbazan Medical and Engineering Research Center with the ethics code of ID IR.ISAAR.REC.1397.015 and has been supported by this research center.
Conflicts of Interests: This article is retrieved from the research project approved by the ethics committee of the Janbazan Medical and Engineering Research Center
Authors' Contribution: Azarmi S. (First Author), Introduction Writer/Main Researcher (20%); Baniyaghoobi F. (Second Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%); Zareiyan A. (Third Author), Methodologist/ Assistant Researcher/Statistical Analyst (20%); Farsi Z. (Furth Author), Methodologist/Assistant Researcher/Statistical Analyst (20%); Safshekan S. (Fifth Author), Assistant Researcher/Discussion Writer (20%)
Funding/Support: The present study was funded by Janbazan Medical and Engineering Research Center.
Discussion
Due to the lack of standard questionnaires to assess adaptation based on the Roy model in veterans with lower limb amputation, the present study aimed to psychometrics of the instrument.
Amputated veterans have problems adapting to their "physiological" dimension due to their chronic illness's physical and psychological effects. According to the Roy Adaptation Model and studies in this field, the questionnaire items in the physiological dimension include five basic physiological needs, including activity and rest, nutrition, defecation, oxygenation, and protection [23]. In the dimension of "self-perception", Roy introduces three cases of self-objectivity, self-personality, and self concerning others [24]. The findings also indicate the importance of personality and psychological characteristics of amputated veterans, self-satisfaction and activities, and interaction with family and community in the dimension of "self-perception". According to Roy, the problems that need to be considered in the "role play" dimension are as follows: 1) Role-playing failure in which a person is unable to perform previous behaviors about her/his role; 2) Role conflict when others' expectations of the individual differ from one's own [24]. The questionnaire items designed in the role-playing dimension also showed the problems of veterans in this dimension; because veterans, depending on their physical and mental condition may have conflicts or inadequacies in the roles and abilities of themselves and others. The "independence/dependency" dimension focuses on how people communicate, their goals, structure, and the extent of their relationships [25]. Problems with this dimension can occur in the following two ways: 1) disorder in being dependent; 2) disorder in being independent. Problems in this dimension may also arise in rejection, aggression, violence, competition, lack of cooperation, and desire to be alone [23]. The items related to this dimension of the questionnaire also focus on the communication and support system veterans.
Based on the research background, it was found that several studies have been performed to evaluate the adaptation based on the Roy Adaptation Pattern in different target groups; in each of these studies, a tool has been used to evaluate and measure the compatibility of patients. In the Kisacık study, investigating nursing interventions based on the Roy adaptation pattern in patients undergoing hemiglossectomy surgery, behaviors of the patients were assessed in four dimensions of Roy adaptation pattern, and objective and subjective information was recorded [26]. This study is consistent with the present study in terms of examining the four dimensions of the Roy model; however, due to the difference in observational behavior and results of the interventions and the research community, it is not consistent with our study. In a study, Kavradim investigated the effect of intervention based on the Roy Adaptation Model by training and telephone follow-up method on the quality of self-efficacy of patients after myocardial infarction. In this study, the Roy Adaptation Scale developed by Calista Roy was used to evaluate the adaptation process [27]. In another study, an instrument was designed to investigate the effect of an educational program based on the Roy Adaptation Model on the adaptation of patients with obstructive pulmonary disease. Like the previous study instrument, it included all the dimensions of the Roy adaptation model. However, the instrument psychometrics was not assessed [15]. Lee et al. used the Roy adaptation model in developing prenatal screening tools [28]. In the designed instrument of Lee et al., all four dimensions of the Roy Adaptation Model have been considered, and the psychometrics of the instrument has been assessed, but their research is different from the present research in terms of the statistical population. In another study performed on diabetic patients, the instrument used was the Roy recognition and recognition form, in which the physiological dimension of the samples was not assessed due to the specific conditions of diabetic patients. Using this form, patients were interviewed [29]. In addition to reviewing the Roy Adaptation Pattern in all four dimensions and performing instrument psychometrics, the instrument is designed to be easier to analyze and requires less time.
Mohammadpour investigated the effect of intervention based on the Roy Adaptation Model on self-perception in first pregnant women. The research instrument was a questionnaire to assess the level of adaptation in the dimension of self-perception based on the Roy Adaptation Model consisting of three areas of "spiritual-moral self, self-stability and expected self" and a total of 22 items ranked on the Likert scale. The instrument of the above study includes only one dimension of the Roy Adaptation Model, and, unlike the present study, the psychometrics of the instrument has not been measured, and the research community is different. Various other studies were conducted to investigate the effect of implementing a care program based on the Roy Adaptation Model on different research units [31-33]. In the mentioned studies, as in the present study, all four dimensions of the Roy Adaptation Model were examined, but these studies are not in accordance with the present study in terms of the research community and the lack of instrument psychometrics. In another study that examined the effect of a care program on the physiological adaptation of type 2 diabetic patients based on the Roy Adaptation Model, the instrument included the descriptive items of Roy's four dimensions [11]. It is difficult to fill out the descriptive questionnaires by patients and nurses, and its analysis requires more time. Therefore, the researchers found it necessary to design an instrument that is easier to analyze and requires less time. So, Hekary, in a study on women with coronary artery disease, used various scales to assess four dimensions of the Roy Adaptation Model [17].
In addition to designing the items based on the Roy Adaptation Model, attempts have been made to address all subscales related to the four dimensions based on the framework of this model, and psychometrics of this model has been performed, which is effective in designing the proper instrument. Efforts were also made to design the objective and behavioral items so that veterans with lower-limb amputations could easily understand and answer them. It is recommended to conduct more research to use this instrument more comprehensively in different clinical centers for veterans and to conduct similar research to design similar instruments for different target groups. Health care professionals, especially nurses, can use this instrument in clinical centers to provide more effective care to veterans with lower limb amputation and take effective steps to improve these patients' adaptation and quality of life.
In such studies, a cumulative variance probability of less than 50% is not unexpected; because the samples may not have the right conditions to respond, and the sample size is limited, which is one of the research limitations.
Conclusion
The designed instrument has the face, content, factor validities, and acceptable reliability, which indicate its suitability for measuring the compatibility of veterans with lower limb amputation based on the Roy Adaptation Model and providing better services in the field of care for these patients.
Acknowledgments: The authors appreciated the participation and cooperation of the officials of the Janbazan Medical and Engineering Research Center, management of Kosar Orthosis and Prosthesis Center, veterans clinics affiliated with this center, and the veterans participating in this research.
Ethical Permissions: This article is retrieved from the research project approved by the ethics committee of the Janbazan Medical and Engineering Research Center with the ethics code of ID IR.ISAAR.REC.1397.015 and has been supported by this research center.
Conflicts of Interests: This article is retrieved from the research project approved by the ethics committee of the Janbazan Medical and Engineering Research Center
Authors' Contribution: Azarmi S. (First Author), Introduction Writer/Main Researcher (20%); Baniyaghoobi F. (Second Author), Introduction Writer/Assistant Researcher/Discussion Writer (20%); Zareiyan A. (Third Author), Methodologist/ Assistant Researcher/Statistical Analyst (20%); Farsi Z. (Furth Author), Methodologist/Assistant Researcher/Statistical Analyst (20%); Safshekan S. (Fifth Author), Assistant Researcher/Discussion Writer (20%)
Funding/Support: The present study was funded by Janbazan Medical and Engineering Research Center.
Keywords:
References
1. Khani H, Joharinia M, Kariminasab MH, Ganji R, Azadmarzabadi E, Shakeri M, et al. Evaluation of quality of life in amputee veterans in Mazandaran. J North Khorasan Univ Med Sci. 2011;3(1):49-56. [Persian] [Link] [DOI:10.29252/jnkums.3.1.8]
2. Naderi A, Sedighi S, Roshanaei G, Ahmadpanah M, Rostampour F, Asadi Z. Quality of life of the spouses of war related amputees of Hamedan city, Iran. TEBE JANBAZ. 2016;8(3):157-63. [Persian] [Link]
3. Rahimi AAF, Masoumi M, Soroush M, Mousavi B. Orthopedic complications in bilateral lower limb amputation. Iran J Orthop Surg. 2009;7(2):58-63. [Persian] [Link]
4. Farsi Z, Azarmi S. Effect of roy's adaptation model-guided education on coping strategies of the veterans with lower extremities amputation: A double-blind randomized controlled clinical trial. International J Community Based Nurs Midwifery. 2016;4(2):127-36. [Link]
5. Masoumi M, Esfandiari E, Yavari A, Saeedi H, Allami M. Consideration of chronic pain and current prosthetic satisfaction in above knee amputees. TEBE JANBAZ. 2011;3(2):53-8. [Persian] [Link]
6. Esfandiari E, Masoumi M, Yavari A, Saeedi H, Allami M. Efficacy of long-term outcomes and prosthesis satisfaction in war related above knee amputees of Tehran in 1387. J Res Rehabil Sci. 2011;7(1). [Persian] [Link]
7. Mousavi B, Mirsalimi F, Soroush MR, Masumi M, Montazeri A. Quality of life in war related bilateral lower limb amputees: Results of a national project from Iran. PAYESH. 2009;8(3):303-10. [Link]
8. Mousavi B, Soroush MR, Montazeri A. Quality of life in chemical warfare survivors with ophthalmologic injuries: The first results form Iran chemical warfare victims health assessment study. Health Qual Life Outcomes. 2009;7:2. [Link] [DOI:10.1186/1477-7525-7-2] [PMID] [PMCID]
9. Azarmi S, Farsi Z. Roy's adaptation model-guided education and promoting the adaptation of veterans with lower extremities amputation. Iran Red Crescent Med J. 2015;17(10):25810. [Link] [DOI:10.5812/ircmj.25810] [PMID] [PMCID]
10. Bastaminia A, Rezaie MR, Saraie MH. Explaining and analyzing the concept of resiliency and its indicators and frameworks in natural disasters. Disaster Prev Manag Knowl. 2016;6(1):32-46. [Persian] [Link]
11. Sadeghnazhad Forotgeh M, Vanaki Z, Memarian R. The effect of nursing care plan based on Roy adaptation model on psychological adaptation in patients with diabetes type II. Evid Based Care J. 2011;1(1):5-20. [Persian] [Link]
12. Roy C. Research based on the Roy adaptation model: Last 25 years. Nurs Sci Q. 2011;24(4):312-20. [Link] [DOI:10.1177/0894318411419218] [PMID]
13. Roy C. Extending the Roy adaptation model to meet changing global needs. Nurs Sci Q. 2011;24(4):345-51. [Link] [DOI:10.1177/0894318411419210] [PMID]
14. Alligood MR. Nursing theory: Utilization & application. Maryland Heights: Mosby; 2013. [Link]
15. Akyil RC, Erguney S. Roy's adaptation model‐guided education for adaptation to chronic obstructive pulmonary disease. J Adv Nurs. 2013;69(5):1063-75. [Link] [DOI:10.1111/j.1365-2648.2012.06093.x] [PMID]
16. Bakan G, Akyol AD. Theory‐guided interventions for adaptation to heart failure. J Adv Nurs. 2008;61(6):596-608. [Link] [DOI:10.1111/j.1365-2648.2007.04489.x] [PMID]
17. Hekari D, Mohammadzadeh R. The assessment of adaptation rate of coronary artery disease female patients according to quadruple aspects of physiologic, self-perception, role playing and independence/dependence in Tabriz, 1386-87. Med Sci J. 2008;18(3):187-93. [Persian] [Link]
18. Azarmi S, Farsi Z, Sajadi SA. Development of adaptation questionnaire using Roy's adaptation model and its psychometrics on veterans with lower limb amputation. HAYAT. 2014;19(4):26-37. [Persian] [Link]
19. Tabachnick BG, Fidell LS. Using multivariate statistics. Boston: Allyn & Bacon; 2001. [Link]
20. Hair JF. Multivariate data analysis. Hoboken: Prentice Hall; 2009. [Link]
21. World medical association. World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-4. [Link] [DOI:10.1001/jama.2013.281053] [PMID]
22. Ebadi A, sharifnia H, Zareiyan A. Scale Development in health science. Tehran: JAMENEGAR; 2019. [Persian] [Link]
23. Dehghan Nayeri N, Jalalinia F. Theorems and nursing theories. Tehran: BOSHRA; 2004. [Persian] [Link]
24. Memarian R. Application of nursing concepts and theories. Tehran: Tarbiat Modarres University; 1999. [Persian] [Link]
25. Alligood MR, Marriner-Tomey A. Nursing Theorists and their work. Maryland Heights: Mosby; 1997. [Link]
26. Gurlek Kisacik O, CigErci Y. Nursing Approach Based on the Roy Adaptation Model in a Patient Undergoing Hemiglossectomy Surgery for Tongue Cancer. Koc Universitesi Hemsirelikte Egitim Arastırma Dergisi. 2019;16(3):268-75. [Turkish] [Link] [DOI:10.5222/HEAD.2019.268]
27. Turan Kavradim S, Canli Ozer Z. The effect of education and telephone follow‐up intervention based on the Roy adaptation model after myocardial infarction: Randomised controlled trial. Scand J Caring Sci. 2020;34(1):247-60. [Link] [DOI:10.1111/scs.12793] [PMID]
28. Lee LYK, Tsang AYK, Wong KF, Lee JKL. Using the Roy adaptation model to develop an antenatal assessment instrument. Nurs Sci Q. 2011;24(4):363-9. [Link] [DOI:10.1177/0894318411419209] [PMID]
29. Mastaelizadeh H, Sheikhi HR, Sheikhi AR. Effect of a nursing intervention based on Roy's adaptation model on adaptation dimensions in patients with type II diabetes mellitus. J Diabetes Nurs. 2018;6(2):452-62. [Persian] [Link]
30. Mohammad Pour A, Najafi S, Tavakkoli Zadeh J, Mohammad Zadeh F. The effect of intervention based on Roy adaptation model on personal self-concept in primi-gravida women. J Sabzevar Univ Med Sci. 2016;22(6):999-1007. [Persian] [Link]
31. Maghsoodi E, Hemmati Maslak Pak M, Naseri O. The effect of care plan application based on Roy's adaptation model on the spiritual well-being of elderly people in Urmia nursing homes. Int J Med Res Health Sci. 2016;5(11):408-14. [Link]
32. Maleki F, Hemmati Maslakpak M, Khalkhali H. Study the effect of performance Roy adaptation model on intensity and effects of fatigue in multiple sclerosis patients. Nurs Midwifery J. 2016;14(6):571-9. [Persian] [Link]
33. Mohammadi K, Mehralian HA, Abolhasani S, Khairi S, Aghabozorgi F. Investigation the effect of program based on Roy's adaptation model on general health of offspring of people with multiple sclerosis. J Clin Nurs Midwifery. 2019;4(3):472-81. [Persian] [Link]