
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

0.5
Cite Score
SJR: 0.129 / SNIP: 0.140
Volume 16, Issue 4 (2024)
Iran J War Public Health 2024, 16(4): 325-331 |
Back to browse issues page
Article Type:
Subject:





Ethics code: LB.02.06/2/655/2023
History
Received: 2024/11/13 | Accepted: 2024/12/16 | Published: 2024/12/18
Received: 2024/11/13 | Accepted: 2024/12/16 | Published: 2024/12/18
How to cite this article
Roza E, Rusdi M, Guspianto G, Hasibuan M. Self-Care Educational Model to Enhance the Elderly with Hypertension. Iran J War Public Health 2024; 16 (4) :325-331
URL: http://ijwph.ir/article-1-1530-en.html
URL: http://ijwph.ir/article-1-1530-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Department of Public Health Sciences, Faculty of Mathematics and Natural Sciences Education, Jambi University, Jambi, Indonesia
2- Department of Chemisrty Education, Faculty of Teacher Training and Education, Jambi University, Jambi, Indonesia
3- Department of Public Health Sciences, Faculty of Medicine and Health Sciences, Jambi University, Jambi, Indonesia
2- Department of Chemisrty Education, Faculty of Teacher Training and Education, Jambi University, Jambi, Indonesia
3- Department of Public Health Sciences, Faculty of Medicine and Health Sciences, Jambi University, Jambi, Indonesia
Full-Text (HTML) (1290 Views)
Introduction
Hypertension, a chronic condition, is the leading cause of cardiovascular-related fatalities [1]. Its global impact is significant, affecting over one billion people, with a prevalence ranging from 30% to 45% [2, 3]. This prevalence continues to rise and is projected to surpass 1.5 billion cases by 2025 [1]. Eshkoor et al. highlighted the considerable prevalence of hypertension among the elderly worldwide [4]. In Indonesia, based on the RISKESDAS data, hypertension prevalence increased from 25.8% in 2013 to 34% in 2018, with rates exceeding 60% among individuals aged 60 and older [5].
Despite the seriousness of this health issue, global adherence to blood pressure monitoring among hypertensive patients remains alarmingly low [6]. Only 12% regularly monitor their blood pressure, and just 8.9% adhere consistently to treatment. This low adherence is attributed to inadequate awareness, compounded by challenges such as limited medication availability, insufficient insurance coverage, and restricted access to healthcare services [7, 8].
The elderly are particularly vulnerable to hypertension and its complications [9]. Alarmingly, evidence indicates that a substantial proportion of hypertensive individuals, especially the elderly, remain undiagnosed, heightening the risk of complications [10]. Uncontrolled hypertension significantly increases the likelihood of cardiovascular, cerebrovascular, and renal complications [11].
Mitigating these risks requires fostering adherence among hypertensive patients. Due to its chronic nature, hypertension necessitates diligent self-management [12]. Essential self-management practices include engaging in physical activity, managing weight, adhering to a healthy diet, managing stress, consistently monitoring blood pressure, attending regular healthcare appointments, and following prescribed medication regimens [13]. The effectiveness of self-care practices in hypertension management is particularly notable among the elderly [14].
Despite the Indonesian government's implementation of several health promotion programs, the prevalence of hypertension in the country has not decreased. Similarly, various studies proposing educational models that utilize technology have achieved limited success in improving compliance among hypertensive patients. Furthermore, while the BPJS Health Program has contributed to hypertension control efforts, only a small proportion of elderly hypertensive individuals benefit from the BPJS Health Prolanis program for hypertension management [15, 16].
Health behaviorists have introduced various theories in the field of health behavior analysis to examine the health behaviors of individuals and communities. Among these, the health belief model (HBM) is one of the most frequently employed. The HBM explores individuals’ beliefs about health behaviors, while social cognitive theory (SCT) emphasizes the role of social support and environmental factors in driving health behavior changes. Notably, health literacy and self-efficacy are critical factors influencing hypertension self-management behaviors among the elderly [17].
Several factors have been identified as influencing the behavior of hypertensive patients, including knowledge, belief in the effectiveness of therapy, self-efficacy, and social support. Hypertension self-management education aims to empower individuals with hypertension to take an active role in managing their condition [18]. The implementation of hypertension self-management education is expected to lead to changes in self-management behaviors among hypertensive patients [19]. Notably, Fletcher et al. observed that self-management interventions can improve compliance with blood pressure control and adherence to hypertension treatment protocols [20]. Additionally, research by Delavar et al. demonstrated that tailored self-management education, which takes health literacy levels into account, significantly enhances treatment adherence among elderly individuals with hypertension [7].
This research introduces significant novelty by developing an innovative objective, cognitive, holistic, and active (OCHA) educational model to improve hypertension self-care among the elderly. This model incorporates a holistic approach grounded in cognitive and objective understanding, specifically designed to optimize hypertension monitoring and management in this population. By adopting an active approach that encourages participants to directly engage in the education and care process, this research has the potential to significantly impact hypertension control—a major health issue among the elderly. Enhancing the knowledge and skills of elderly individuals to independently manage hypertension can reduce the risk of severe complications such as stroke, heart disease, and kidney failure, while also alleviating the burden of long-term healthcare costs. This study aimed to develop and evaluate an effective educational model to improve self-care practices among elderly individuals with hypertension.
Materials and Methods
Study design
This experimental study employed the pre-test and post-test measures to evaluate changes in knowledge before and after the intervention and was conducted from March to June 2024. A pilot test was conducted with a randomly selected group of elderly participants to assess the effectiveness of the developed educational model.
The research adopted a research and development (R&D) approach, utilizing the ADDIE model framework, which consists of five sequential stages, namely analysis, design, development, implementation, and evaluation. The ADDIE model facilitates iterative evaluation and refinement throughout each stage of development. This study presents the OCHA model syntax (orientation, challenges and concerns, health content delivery, awareness around behavior and environment), which represents an innovative paradigm in health education interventions for older individuals with hypertension. The conceptual framework of this model, which provides a comprehensive approach to addressing health behaviors, is derived from the SCT and the HBM.
Subjects
The process of selecting research respondents involved several stages. Initially, a single urban village in Jambi City was selected as the study area. Respondents from this village were then randomly chosen. The respondents consisted of 30 elderly individuals, randomly selected from the community or related health institutions. Based on calculations using Slovin's formula with a margin of error of 5%, a sample size of 30 individuals corresponds to a population size of 32 individuals. This suggests that nearly the entire population will be included in the study, given the very high proportion of the sample relative to the total population.
The inclusion criteria required participants to be aged 60 years or older, have a medical diagnosis of hypertension, and be willing to participate in the full series of educational programs and complete a knowledge questionnaire on hypertension management. Elderly individuals with cognitive impairments or other chronic illnesses that could hinder their understanding of the material were excluded. The random selection of respondents was intended to ensure diverse characteristics representative of the elderly population, thereby enhancing the generalizability of the findings to improve hypertension management among elderly individuals in various settings.
Data collection
Data collection was carried out using a validated questionnaire designed to assess the knowledge of elderly individuals about hypertension management. The questionnaire included questions on hypertension, its management, risk factors, and strategies to prevent hypertension-related complications. Prior to the intervention, a pre-test was administered to assess respondents' baseline knowledge. After the educational program, which included counseling on hypertension and self-care techniques, the same questionnaire was used to measure changes in knowledge through a post-test. This data collection process was conducted in a single session for each respondent, with the questionnaires completed individually under the supervision of a trained facilitator.
Model development
In alignment with the principles of Geragogy theory, the selected educational media is tailored to meet the needs of the elderly population by employing direct explanations, clear imagery, and accessible language. This approach is realized through lectures or audio-visual media, such as videos. The study establishes a standardized process for synthesizing theory and implementing educational interventions, which is meticulously documented in a written script.
During the analysis stage, the fundamental elements of the intervention design and development process are examined, including problem analysis, contextual analysis, and literature review. The problem/needs analysis was conducted to address both theoretical and practical issues observed empirically in the field. Contextual analysis involved field visits to identify specific factors, facilitating the prediction of product interactions with the target audience for easier design. Literature analysis involved reviewing relevant theories to build a conceptual framework for determining the design principles to be applied.
Once the analysis results were deemed feasible, researchers proceeded to design and develop products that addressed the identified problems. The intervention design produced at this stage was then refined based on feedback from expert and practitioner validation. Evaluation involved reviewing the design, development, and analysis processes to ensure that the intervention is ready for testing.
Instrument
The validity test of the knowledge questionnaire was conducted to ensure that the instrument accurately measured elderly individuals' knowledge regarding hypertension management. A panel of specialists, including geriatricians and medical professionals, evaluated the content validity of the original questionnaire, which consisted of twelve items. The results indicated that ten of the questions demonstrated good validity, while two were deemed invalid due to their irrelevance or lack of clarity in measuring the intended knowledge. Based on feedback from the expert panel, the two invalid questions were replaced with more appropriate and relevant items. Following these revisions, the updated questionnaire, now containing ten valid items, was used for data collection. A final validity test showed that all questionnaire items had validity coefficients exceeding 0.7, confirming the instrument's validity for measuring elderly knowledge in this study.
Statistical analysis
Data analysis was performed to evaluate changes in elderly participants' knowledge of hypertension management after participating in the educational program. Prior to statistical testing, a normality test was conducted to ensure that the pre-test and post-test knowledge data were normally distributed. The Kolmogorov-Smirnov and Shapiro-Wilk tests were used, and the results indicated that the knowledge data followed a normal distribution, with p-values greater than 0.05 for both tests. Given the normal distribution of the data, a paired sample t-test was applied to assess significant differences in knowledge scores before and after the educational intervention. This test compared the mean pre-test and post-test scores of the same respondents. If the test results showed a p-value <0.05, the results were considered statistically significant. The data were analyzed using SPSS software version 23.0.
Findings
At the design stage, the researchers developed and constructed products to address the identified problems by creating a storyboard consisting of sequential narratives with explanatory textual and visual information for the development of educational models. This storyboard then served as the initial prototype for developing an audiovisual model in the form of an educational video.
The storyboard for the development of the educational model aimed at enhancing knowledge and self-management of hypertension in the elderly. It was structured across 14 slides, each focusing on critical aspects of hypertension management. The session began with an introduction to hypertension self-management education, followed by an overview of hypertension, its classification, and risk factors. Subsequent slides covered the epidemiology of hypertension, with particular attention to its impact on older adults. Respondents were able to easily use the educational media and demonstrated a better understanding after using it (Table 1).
Table 1. One-on-one trial results

The results of the one-on-one evaluation indicated that the educational model was comprehensible and engaging for the elderly. Furthermore, the educational video was found to be both interesting and useful for them (Table 2).
Table 2. Interview results on one-on-one trial

In the small group trial, respondents found it easier to use the media and expressed interest in using it (Table 3).
Table 3. Small group trial results
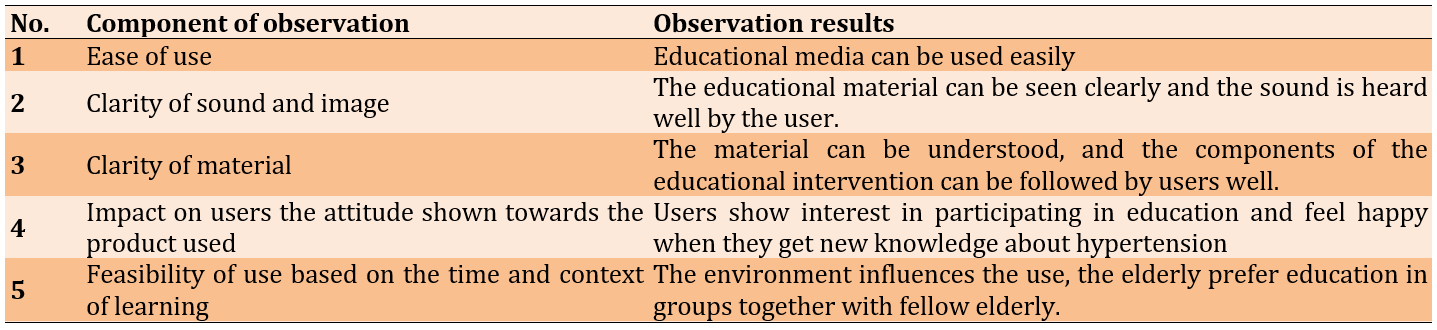
Interviews with 13 respondents in the small group trial indicated that they found the material easy to understand after using the media and were interested in using it due to its features (Table 4).
Table 4. Interview results on small group trial

The data analysis examined changes in elderly participants' knowledge of hypertension management before and after participating in the educational intervention. The mean pre-test knowledge score was 42.00±5.20. After completing the educational program, the mean knowledge score increased to 68.00±4.50. The median score also showed improvement, rising from 43.00 in the pre-test to 69.00 post-intervention, indicating a consistent increase in knowledge across respondents. The statistical significance of the difference between the pre-test and post-test scores was confirmed by the paired t-test analysis (p<0.05). These findings demonstrated that the educational program successfully enhanced the older participants' understanding of managing their hypertension.
Discussion
This study aimed to develop and evaluate an effective educational model to improve self-care practices among elderly individuals with hypertension. The definition of hypertension, risk factors, clinical symptoms, complications, management strategies, the role of the environment, and the use of JKN in managing hypertension were identified as essential educational materials for the elderly, according to the needs analysis from the first survey. The elderly preferred information that could be seen and heard directly, as they had difficulty reading text on leaflets. This preference aligns with feedback from the person in charge of the Elderly Program at the Health Office and the PUSKESMAS, which indicates that hypertension education media have primarily been in the form of leaflets provided by the Ministry of Health. Our findings serve as a guide for developing educational models for older adults with hypertension, addressing their unique issues and requirements through the creation of relevant materials and the use of appropriate educational media.
The design and development of the educational model followed the analytical stage. The educational model for self-management of hypertension in the elderly, developed using a Geragogy approach, consisted of four intervention components. These educational intervention activities aligned with the theoretical constructs synthesized to improve the self-management of hypertension. A storyboard was then created and developed into a prototype using audiovisual media in the form of educational videos based on the Geragogy approach.
These experts provided in-depth insights into the essential concepts and appropriate teaching methods for the elderly, ensuring that the educational model addresses critical aspects of hypertension self-management. They evaluated whether the learning materials and methods are suitable for the elderly and confirmed that the educational model aligns with their needs. Additionally, they assessed the educational approach's appropriateness in relation to the culture, environment, and social conditions of the elderly. This validation helped determine the effectiveness of the educational model in achieving its goals, such as improving hypertension self-management among the elderly.
The educational model developed was in the form of audiovisual media, allowing the developer to measure elderly users' comfort with this format during the evaluation stage. Two indicators were assessed, including perceived usefulness, which measured how beneficial users believe the audiovisual educational model is for elderly individuals with hypertension, and perceived ease of use, which evaluated how easily users understand and use the audiovisual media to improve hypertension self-management. This evaluation also helps identify barriers that users may face when using the media.
The educational intervention improved participants' understanding of hypertension and their ability to control it. These results provide important information on the effectiveness of health education programs for senior citizens. For older individuals with hypertension, adequate blood pressure control, medication adherence, and lifestyle changes all depend on having a sufficient understanding of hypertension and how to manage it [21]. These results are consistent with other research that found hypertension knowledge, attitudes, and practices post-test scores are higher than pre-test levels [22].
The increase in medication adherence, and in some cases, the ability to enhance self-efficacy and self-care in patients by sending encouraging messages about hypertension management via an Android application [23, 24], has been observed.
Our study suggests that a model-based educational intervention tailored to the conditions of the elderly has the potential to enhance self-management practices. Therefore, our findings support the effectiveness of health education interventions, corroborating previous studies that have reported improvements in hypertension self-care practices among elderly patients [22, 25].
This study is notable for its novel approach to health education interventions, which were specifically created to address the unique needs and concerns of older adults with hypertension. The results may also help the government implement educational initiatives to raise awareness among senior citizens with hypertension. These results align with those of earlier research [25]. The theory-based educational intervention was incorporated into the development of a comprehensive OCHA model. This study is the first to evaluate how a model-based health education intervention impacts the knowledge and self-management of hypertension in the targeted senior population with hypertension.
A study on the effectiveness of m-Health was conducted by Bozorgi et al. [26] using a mobile application-based educational-supportive intervention, alongside routine treatment. The content and features of the application were developed based on the educational needs of hypertensive patients. They reported an increase in medication adherence in the intervention group compared to the control group, and an improvement in adherence to a low-fat, low-salt diet, as well as moderate physical activity in the intervention group.
A limitation of this study is the relatively small sample size, which, although adequate to meet the study’s minimal requirements, may impact the generalizability of the findings. Additionally, the brief study period, which focused on changes in hypertension self-management techniques, restricts our ability to assess the long-term effects of the intervention. By employing a structured approach that delivers clear and easy-to-understand information, this educational model has successfully improved older adults' knowledge of hypertension management while also enhancing their self-care skills.
Conclusion
The development of an effective educational model has the potential to significantly improve self-care practices among the elderly with hypertension, thereby supporting better health management in this population.
Acknowledgments: The authors would like to thank all participants for their cooperation and involvement throughout the study. They also express their gratitude to the Head of Jambi University for their support and assistance. The researchers, data collection team, enumerator team, and all parties involved in this project are sincerely appreciated.
Ethical Permissions: Participants' privacy was protected, and there was no incentive to participate in the study. Registered prospective respondents signed an informed consent form. Ethical permission was obtained before data collection began. According to the authors, this study was authorized by the Jambi University Health Research Ethics Council and complied with all ethical clearance procedures (LB.02.06/2/655/2023).
Conflicts of Interests: The authors declared no conflicts of interests.
Authors' Contribution: Roza E (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer/Statistical Analyst (40%); Rusdi M (Second Author), Assistant Researcher/Discussion Writer/Statistical Analyst (20%); Guspianto G (Third Author), Introduction Writer/Methodologist/Assistant Researcher (20%); Hasibuan MHE (Fourth Author), Assistant Researcher/Discussion Writer/Statistical Analyst (20%)
Funding/Support: No funding was received.
Hypertension, a chronic condition, is the leading cause of cardiovascular-related fatalities [1]. Its global impact is significant, affecting over one billion people, with a prevalence ranging from 30% to 45% [2, 3]. This prevalence continues to rise and is projected to surpass 1.5 billion cases by 2025 [1]. Eshkoor et al. highlighted the considerable prevalence of hypertension among the elderly worldwide [4]. In Indonesia, based on the RISKESDAS data, hypertension prevalence increased from 25.8% in 2013 to 34% in 2018, with rates exceeding 60% among individuals aged 60 and older [5].
Despite the seriousness of this health issue, global adherence to blood pressure monitoring among hypertensive patients remains alarmingly low [6]. Only 12% regularly monitor their blood pressure, and just 8.9% adhere consistently to treatment. This low adherence is attributed to inadequate awareness, compounded by challenges such as limited medication availability, insufficient insurance coverage, and restricted access to healthcare services [7, 8].
The elderly are particularly vulnerable to hypertension and its complications [9]. Alarmingly, evidence indicates that a substantial proportion of hypertensive individuals, especially the elderly, remain undiagnosed, heightening the risk of complications [10]. Uncontrolled hypertension significantly increases the likelihood of cardiovascular, cerebrovascular, and renal complications [11].
Mitigating these risks requires fostering adherence among hypertensive patients. Due to its chronic nature, hypertension necessitates diligent self-management [12]. Essential self-management practices include engaging in physical activity, managing weight, adhering to a healthy diet, managing stress, consistently monitoring blood pressure, attending regular healthcare appointments, and following prescribed medication regimens [13]. The effectiveness of self-care practices in hypertension management is particularly notable among the elderly [14].
Despite the Indonesian government's implementation of several health promotion programs, the prevalence of hypertension in the country has not decreased. Similarly, various studies proposing educational models that utilize technology have achieved limited success in improving compliance among hypertensive patients. Furthermore, while the BPJS Health Program has contributed to hypertension control efforts, only a small proportion of elderly hypertensive individuals benefit from the BPJS Health Prolanis program for hypertension management [15, 16].
Health behaviorists have introduced various theories in the field of health behavior analysis to examine the health behaviors of individuals and communities. Among these, the health belief model (HBM) is one of the most frequently employed. The HBM explores individuals’ beliefs about health behaviors, while social cognitive theory (SCT) emphasizes the role of social support and environmental factors in driving health behavior changes. Notably, health literacy and self-efficacy are critical factors influencing hypertension self-management behaviors among the elderly [17].
Several factors have been identified as influencing the behavior of hypertensive patients, including knowledge, belief in the effectiveness of therapy, self-efficacy, and social support. Hypertension self-management education aims to empower individuals with hypertension to take an active role in managing their condition [18]. The implementation of hypertension self-management education is expected to lead to changes in self-management behaviors among hypertensive patients [19]. Notably, Fletcher et al. observed that self-management interventions can improve compliance with blood pressure control and adherence to hypertension treatment protocols [20]. Additionally, research by Delavar et al. demonstrated that tailored self-management education, which takes health literacy levels into account, significantly enhances treatment adherence among elderly individuals with hypertension [7].
This research introduces significant novelty by developing an innovative objective, cognitive, holistic, and active (OCHA) educational model to improve hypertension self-care among the elderly. This model incorporates a holistic approach grounded in cognitive and objective understanding, specifically designed to optimize hypertension monitoring and management in this population. By adopting an active approach that encourages participants to directly engage in the education and care process, this research has the potential to significantly impact hypertension control—a major health issue among the elderly. Enhancing the knowledge and skills of elderly individuals to independently manage hypertension can reduce the risk of severe complications such as stroke, heart disease, and kidney failure, while also alleviating the burden of long-term healthcare costs. This study aimed to develop and evaluate an effective educational model to improve self-care practices among elderly individuals with hypertension.
Materials and Methods
Study design
This experimental study employed the pre-test and post-test measures to evaluate changes in knowledge before and after the intervention and was conducted from March to June 2024. A pilot test was conducted with a randomly selected group of elderly participants to assess the effectiveness of the developed educational model.
The research adopted a research and development (R&D) approach, utilizing the ADDIE model framework, which consists of five sequential stages, namely analysis, design, development, implementation, and evaluation. The ADDIE model facilitates iterative evaluation and refinement throughout each stage of development. This study presents the OCHA model syntax (orientation, challenges and concerns, health content delivery, awareness around behavior and environment), which represents an innovative paradigm in health education interventions for older individuals with hypertension. The conceptual framework of this model, which provides a comprehensive approach to addressing health behaviors, is derived from the SCT and the HBM.
Subjects
The process of selecting research respondents involved several stages. Initially, a single urban village in Jambi City was selected as the study area. Respondents from this village were then randomly chosen. The respondents consisted of 30 elderly individuals, randomly selected from the community or related health institutions. Based on calculations using Slovin's formula with a margin of error of 5%, a sample size of 30 individuals corresponds to a population size of 32 individuals. This suggests that nearly the entire population will be included in the study, given the very high proportion of the sample relative to the total population.
The inclusion criteria required participants to be aged 60 years or older, have a medical diagnosis of hypertension, and be willing to participate in the full series of educational programs and complete a knowledge questionnaire on hypertension management. Elderly individuals with cognitive impairments or other chronic illnesses that could hinder their understanding of the material were excluded. The random selection of respondents was intended to ensure diverse characteristics representative of the elderly population, thereby enhancing the generalizability of the findings to improve hypertension management among elderly individuals in various settings.
Data collection
Data collection was carried out using a validated questionnaire designed to assess the knowledge of elderly individuals about hypertension management. The questionnaire included questions on hypertension, its management, risk factors, and strategies to prevent hypertension-related complications. Prior to the intervention, a pre-test was administered to assess respondents' baseline knowledge. After the educational program, which included counseling on hypertension and self-care techniques, the same questionnaire was used to measure changes in knowledge through a post-test. This data collection process was conducted in a single session for each respondent, with the questionnaires completed individually under the supervision of a trained facilitator.
Model development
In alignment with the principles of Geragogy theory, the selected educational media is tailored to meet the needs of the elderly population by employing direct explanations, clear imagery, and accessible language. This approach is realized through lectures or audio-visual media, such as videos. The study establishes a standardized process for synthesizing theory and implementing educational interventions, which is meticulously documented in a written script.
During the analysis stage, the fundamental elements of the intervention design and development process are examined, including problem analysis, contextual analysis, and literature review. The problem/needs analysis was conducted to address both theoretical and practical issues observed empirically in the field. Contextual analysis involved field visits to identify specific factors, facilitating the prediction of product interactions with the target audience for easier design. Literature analysis involved reviewing relevant theories to build a conceptual framework for determining the design principles to be applied.
Once the analysis results were deemed feasible, researchers proceeded to design and develop products that addressed the identified problems. The intervention design produced at this stage was then refined based on feedback from expert and practitioner validation. Evaluation involved reviewing the design, development, and analysis processes to ensure that the intervention is ready for testing.
Instrument
The validity test of the knowledge questionnaire was conducted to ensure that the instrument accurately measured elderly individuals' knowledge regarding hypertension management. A panel of specialists, including geriatricians and medical professionals, evaluated the content validity of the original questionnaire, which consisted of twelve items. The results indicated that ten of the questions demonstrated good validity, while two were deemed invalid due to their irrelevance or lack of clarity in measuring the intended knowledge. Based on feedback from the expert panel, the two invalid questions were replaced with more appropriate and relevant items. Following these revisions, the updated questionnaire, now containing ten valid items, was used for data collection. A final validity test showed that all questionnaire items had validity coefficients exceeding 0.7, confirming the instrument's validity for measuring elderly knowledge in this study.
Statistical analysis
Data analysis was performed to evaluate changes in elderly participants' knowledge of hypertension management after participating in the educational program. Prior to statistical testing, a normality test was conducted to ensure that the pre-test and post-test knowledge data were normally distributed. The Kolmogorov-Smirnov and Shapiro-Wilk tests were used, and the results indicated that the knowledge data followed a normal distribution, with p-values greater than 0.05 for both tests. Given the normal distribution of the data, a paired sample t-test was applied to assess significant differences in knowledge scores before and after the educational intervention. This test compared the mean pre-test and post-test scores of the same respondents. If the test results showed a p-value <0.05, the results were considered statistically significant. The data were analyzed using SPSS software version 23.0.
Findings
At the design stage, the researchers developed and constructed products to address the identified problems by creating a storyboard consisting of sequential narratives with explanatory textual and visual information for the development of educational models. This storyboard then served as the initial prototype for developing an audiovisual model in the form of an educational video.
The storyboard for the development of the educational model aimed at enhancing knowledge and self-management of hypertension in the elderly. It was structured across 14 slides, each focusing on critical aspects of hypertension management. The session began with an introduction to hypertension self-management education, followed by an overview of hypertension, its classification, and risk factors. Subsequent slides covered the epidemiology of hypertension, with particular attention to its impact on older adults. Respondents were able to easily use the educational media and demonstrated a better understanding after using it (Table 1).
Table 1. One-on-one trial results
The results of the one-on-one evaluation indicated that the educational model was comprehensible and engaging for the elderly. Furthermore, the educational video was found to be both interesting and useful for them (Table 2).
Table 2. Interview results on one-on-one trial
In the small group trial, respondents found it easier to use the media and expressed interest in using it (Table 3).
Table 3. Small group trial results
Interviews with 13 respondents in the small group trial indicated that they found the material easy to understand after using the media and were interested in using it due to its features (Table 4).
Table 4. Interview results on small group trial
The data analysis examined changes in elderly participants' knowledge of hypertension management before and after participating in the educational intervention. The mean pre-test knowledge score was 42.00±5.20. After completing the educational program, the mean knowledge score increased to 68.00±4.50. The median score also showed improvement, rising from 43.00 in the pre-test to 69.00 post-intervention, indicating a consistent increase in knowledge across respondents. The statistical significance of the difference between the pre-test and post-test scores was confirmed by the paired t-test analysis (p<0.05). These findings demonstrated that the educational program successfully enhanced the older participants' understanding of managing their hypertension.
Discussion
This study aimed to develop and evaluate an effective educational model to improve self-care practices among elderly individuals with hypertension. The definition of hypertension, risk factors, clinical symptoms, complications, management strategies, the role of the environment, and the use of JKN in managing hypertension were identified as essential educational materials for the elderly, according to the needs analysis from the first survey. The elderly preferred information that could be seen and heard directly, as they had difficulty reading text on leaflets. This preference aligns with feedback from the person in charge of the Elderly Program at the Health Office and the PUSKESMAS, which indicates that hypertension education media have primarily been in the form of leaflets provided by the Ministry of Health. Our findings serve as a guide for developing educational models for older adults with hypertension, addressing their unique issues and requirements through the creation of relevant materials and the use of appropriate educational media.
The design and development of the educational model followed the analytical stage. The educational model for self-management of hypertension in the elderly, developed using a Geragogy approach, consisted of four intervention components. These educational intervention activities aligned with the theoretical constructs synthesized to improve the self-management of hypertension. A storyboard was then created and developed into a prototype using audiovisual media in the form of educational videos based on the Geragogy approach.
These experts provided in-depth insights into the essential concepts and appropriate teaching methods for the elderly, ensuring that the educational model addresses critical aspects of hypertension self-management. They evaluated whether the learning materials and methods are suitable for the elderly and confirmed that the educational model aligns with their needs. Additionally, they assessed the educational approach's appropriateness in relation to the culture, environment, and social conditions of the elderly. This validation helped determine the effectiveness of the educational model in achieving its goals, such as improving hypertension self-management among the elderly.
The educational model developed was in the form of audiovisual media, allowing the developer to measure elderly users' comfort with this format during the evaluation stage. Two indicators were assessed, including perceived usefulness, which measured how beneficial users believe the audiovisual educational model is for elderly individuals with hypertension, and perceived ease of use, which evaluated how easily users understand and use the audiovisual media to improve hypertension self-management. This evaluation also helps identify barriers that users may face when using the media.
The educational intervention improved participants' understanding of hypertension and their ability to control it. These results provide important information on the effectiveness of health education programs for senior citizens. For older individuals with hypertension, adequate blood pressure control, medication adherence, and lifestyle changes all depend on having a sufficient understanding of hypertension and how to manage it [21]. These results are consistent with other research that found hypertension knowledge, attitudes, and practices post-test scores are higher than pre-test levels [22].
The increase in medication adherence, and in some cases, the ability to enhance self-efficacy and self-care in patients by sending encouraging messages about hypertension management via an Android application [23, 24], has been observed.
Our study suggests that a model-based educational intervention tailored to the conditions of the elderly has the potential to enhance self-management practices. Therefore, our findings support the effectiveness of health education interventions, corroborating previous studies that have reported improvements in hypertension self-care practices among elderly patients [22, 25].
This study is notable for its novel approach to health education interventions, which were specifically created to address the unique needs and concerns of older adults with hypertension. The results may also help the government implement educational initiatives to raise awareness among senior citizens with hypertension. These results align with those of earlier research [25]. The theory-based educational intervention was incorporated into the development of a comprehensive OCHA model. This study is the first to evaluate how a model-based health education intervention impacts the knowledge and self-management of hypertension in the targeted senior population with hypertension.
A study on the effectiveness of m-Health was conducted by Bozorgi et al. [26] using a mobile application-based educational-supportive intervention, alongside routine treatment. The content and features of the application were developed based on the educational needs of hypertensive patients. They reported an increase in medication adherence in the intervention group compared to the control group, and an improvement in adherence to a low-fat, low-salt diet, as well as moderate physical activity in the intervention group.
A limitation of this study is the relatively small sample size, which, although adequate to meet the study’s minimal requirements, may impact the generalizability of the findings. Additionally, the brief study period, which focused on changes in hypertension self-management techniques, restricts our ability to assess the long-term effects of the intervention. By employing a structured approach that delivers clear and easy-to-understand information, this educational model has successfully improved older adults' knowledge of hypertension management while also enhancing their self-care skills.
Conclusion
The development of an effective educational model has the potential to significantly improve self-care practices among the elderly with hypertension, thereby supporting better health management in this population.
Acknowledgments: The authors would like to thank all participants for their cooperation and involvement throughout the study. They also express their gratitude to the Head of Jambi University for their support and assistance. The researchers, data collection team, enumerator team, and all parties involved in this project are sincerely appreciated.
Ethical Permissions: Participants' privacy was protected, and there was no incentive to participate in the study. Registered prospective respondents signed an informed consent form. Ethical permission was obtained before data collection began. According to the authors, this study was authorized by the Jambi University Health Research Ethics Council and complied with all ethical clearance procedures (LB.02.06/2/655/2023).
Conflicts of Interests: The authors declared no conflicts of interests.
Authors' Contribution: Roza E (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer/Statistical Analyst (40%); Rusdi M (Second Author), Assistant Researcher/Discussion Writer/Statistical Analyst (20%); Guspianto G (Third Author), Introduction Writer/Methodologist/Assistant Researcher (20%); Hasibuan MHE (Fourth Author), Assistant Researcher/Discussion Writer/Statistical Analyst (20%)
Funding/Support: No funding was received.
Keywords:
References
1. Moradi M, Nasiri M, Jahanshahi M, Hajiahmadi M. The effects of a self-management program based on the 5 A's model on self-efficacy among older men with hypertension. Nurs Midwifery Stud. 2019;8(1):21-7. [Link] [DOI:10.4103/nms.nms_97_17]
2. Kurt D, Gurdogan EP. The effect of self-management support on knowledge level, treatment compliance and self-care management in patients with hypertension. Aust J Adv Nurs. 2022;39(3):14-23. [Link] [DOI:10.37464/2020.393.543]
3. Irwan AM, Potempa K, Abikusno N, Syahrul S. Self-care management for hypertension in Southeast Asia: A scoping review. J Multidiscip Healthc. 2022;15:2015-32. [Link] [DOI:10.2147/JMDH.S367638]
4. Eshkoor SA, Hamid TA, Shahar S, Ng CK, Mun CY. Factors affecting hypertension among the Malaysian elderly. J Cardiovasc Dev Dis. 2016;3(1):8. [Link] [DOI:10.3390/jcdd3010008]
5. Kemenkes RI. Main results of RISKESDAS 2018 [Internet]. Jakarta: KEMENTERIAN KESEHATAN REPUBLIK INDONESIA; 2018 [cited 2022 Jun 20]. Available from: https://repository.dinus.ac.id/docs/ajar/hasil-riskesdas-2018.pdf. [Indonesian] [Link]
6. Gebremichael GB, Berhe KK, Zemichael TM. Uncontrolled hypertension and associated factors among adult hypertensive patients in Ayder comprehensive specialized hospital, Tigray, Ethiopia, 2018. BMC Cardiovasc Disord. 2019;19(1):121. [Link] [DOI:10.1186/s12872-019-1091-6]
7. Delavar F, Pashaeypoor S, Negarandeh R. The effects of self-management education tailored to health literacy on medication adherence and blood pressure control among elderly people with primary hypertension: A randomized controlled trial. Patient Educ Couns. 2020;103(2):336-42. [Link] [DOI:10.1016/j.pec.2019.08.028]
8. Kear T, Harrington M, Bhattacharya A. Partnering with patients using social media to develop a hypertension management instrument. J Am Soc Hypertens. 2015;9(9):725-34. [Link] [DOI:10.1016/j.jash.2015.07.006]
9. Thawornchaisit P, De Looze F, Reid CM, Seubsman S, Tran TT, Banks E, et al. Health-risk factors and the prevalence of chronic kidney disease: Cross-sectional findings from a national cohort of 87 143 Thai open university students. Glob J Health Sci. 2015;7(5):59-72. [Link] [DOI:10.5539/gjhs.v7n5p59]
10. Kaczorowski J, Chambers LW, Karwalajtys T, Dolovich L, Thabane L, Tu K, et al. Cardiovascular health awareness program (CHAP): A community cluster-randomised trial among elderly Canadians. Prev Med. 2008;46(6):537-44. [Link] [DOI:10.1016/j.ypmed.2008.02.005]
11. Susanto RB, Nurmala I, Fatah MZ. The effectiveness of social media on hypertension self-management: A systematic review. J Endur. 2023;8(1):18-29. [Link] [DOI:10.22216/jen.v8i1.1850]
12. McGowan PT. Self-management education and support in chronic disease management. Prim Care. 2012;39(2):307-25. [Link] [DOI:10.1016/j.pop.2012.03.005]
13. Flynn SJ, Ameling JM, Hill-Briggs F, Wolff JL, Bone LR, Levine DM, et al. Facilitators and barriers to hypertension self-management in urban African Americans: Perspectives of patients and family members. Patient Prefer Adherence. 2013;7:741-9. [Link] [DOI:10.2147/PPA.S46517]
14. Klymko KW, Artinian NT, Peters RM, Lichtenberg PA. Personal characteristics and cognition in older African-Americans with hypertension. J Natl Black Nurses Assoc. 2011;22(2):1-10. [Link]
15. Ashari MR, Mukrimin M. Analysis of the economic loss of hypertension sufferers with comorbidities of BPJS participants in the inpatient unit of Budi Agung Hospital, Palu City. J Health Educ Lit. 2022;5(1):40-8. [Indonesian] [Link] [DOI:10.31605/j-healt.v5i1.1737]
16. Latifah I, Maryati H. Analysis of the implementation of the BPJS health chronic disease management program (prolanis) for hypertension patients at the Tegal Gundil Health Center UPTD, Bogor City. HEARTY JURNAL KESEHATAN MASYARAKAT. 2018;6(2). [Indonesian] [Link] [DOI:10.32832/hearty.v6i2.1277]
17. Ongkulna K, Pothiban L, Panuthai S, Chintanawat R. Enhancing self-management through Geragogy-based education in older adults with uncontrolled hypertension: A randomized controlled trial. Pac Rim Int J Nurs Res. 2022;26(4):690-705. [Link]
18. Bachrun E, Murti B, Wijaya M, Sulaeman ES. Health promotion model on preventive behaviors of risk factors for adults' metabolic syndrome in Ponorogo, Indonesia. Glob J Health Sci. 2024;13(4):132-7. [Link] [DOI:10.5539/gjhs.v13n4p132]
19. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the eighth joint national committee (JNC 8). JAMA. 2014;311(5):507-20. [Link] [DOI:10.1001/jama.2013.284427]
20. Fletcher E, Leech R, Mcnaughton SA, Dunstan DW, Lacy KE, Salmon J. Is the relationship between sedentary behaviour and cardiometabolic health in adolescents independent of dietary intake? A systematic review. Obes Rev. 2015;16(9):795-805. [Link] [DOI:10.1111/obr.12302]
21. Chotisiri L, Yamarat K, Taneepanichskul S. Exploring knowledge, attitudes, and practices toward older adults with hypertension in primary care. J Multidiscip Healthc. 2016;9:559-64. [Link] [DOI:10.2147/JMDH.S112368]
22. Roopa KS, Rama Devi G. Impact of intervention programme on knowledge, attitude, practices in the management of hypertension among elderly. Stud Home Community Sci. 2014;8(1):11-6. [Link] [DOI:10.1080/09737189.2014.11885411]
23. Faridi Z, Liberti L, Shuval K, Northrup V, Ali A, Katz DL. Evaluating the impact of mobile telephone technology on type 2 diabetic patients' self‐management: The NICHE pilot study. J Eval Clin Pract. 2008;14(3):465-9. [Link] [DOI:10.1111/j.1365-2753.2007.00881.x]
24. Anglada‐Martinez H, Riu‐Viladoms G, Martin‐Conde M, Rovira‐Illamola M, Sotoca‐Momblona JM, Codina‐Jane C. Does mHealth increase adherence to medication? Results of a systematic review. Int J Clin Pract. 2015;69(1):9-32. [Link] [DOI:10.1111/ijcp.12582]
25. Beigi MAB, Zibaeenezhad MJ, Aghasadeghi K, Jokar A, Shekarforoush S, Khazraei H. The effect of educational programs on hypertension management. Int Cardiovasc Res J. 2014;8(3):94-8. [Link]
26. Bozorgi A, Hosseini H, Eftekhar H, Majdzadeh R, Yoonessi A, Ramezankhani A, et al. The effect of the mobile "blood pressure management application" on hypertension self-management enhancement: A randomized controlled trial. Trials. 2021;22(1):413. [Link] [DOI:10.1186/s13063-021-05270-0]