
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

0.5
Cite Score
SJR: 0.129 / SNIP: 0.140
Volume 16, Issue 4 (2024)
Iran J War Public Health 2024, 16(4): 309-317 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2024/10/31 | Accepted: 2024/12/10 | Published: 2024/12/20
Received: 2024/10/31 | Accepted: 2024/12/10 | Published: 2024/12/20
How to cite this article
Zibasokhan S, Teymouri F, Sharififar S, Azizi M. Factors Influencing the Integrated Management of Chemical Terrorist Incidents. Iran J War Public Health 2024; 16 (4) :309-317
URL: http://ijwph.ir/article-1-1519-en.html
URL: http://ijwph.ir/article-1-1519-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Department of Health in Disasters and Emergencies, Faculty of Nursing, Aja University of Medical Sciences, Tehran, Iran
Full-Text (HTML) (380 Views)
Introduction
In the modern world, due to the growing diversity of chemical production and their global application in various aspects of life, the risk of human exposure to chemicals and their associated health consequences has significantly increased [1]. Chemical accidents are recognized as serious threats [2]. The World Health Organization (WHO) defines a chemical incident as "an uncontrolled release of a toxic substance that has the potential to result in harm to public health and the environment" [3]. These incidents may occur not only as a result of industrial and domestic accidents or natural disasters but also due to intentional releases and terrorist activities [2, 4].
In recent years, threats arising from the use of chemical substances in terrorist operations have become critical security concerns at the international level. Due to their capacity to cause extensive harm, induce profound psychological effects on societies, and their relative accessibility, these materials have attracted the attention of various terrorist groups [5, 6]. Recent studies indicate a significant rise in terrorist chemical attacks over the past five decades, underscoring the need for more detailed analyses [6, 7].
The use of chemical weapons in terrorism is not a new phenomenon and has been documented throughout history. Examples date back to ancient times. In the last century, chemical agents have been employed in numerous wars [8]. The first widespread use of chemical weapons occurred during World War I when Germany utilized chlorine and mustard gas, leading to the death and injury of thousands of soldiers [9, 10].
During the Iran-Iraq War (1980–1988), there was substantial evidence of the Iraqi army’s extensive use of chemical weapons, including sulfur mustard, nerve agents, and other toxic substances [11]. Reports from the Iran-Iraq War recorded 398,587 victims among veterans, with 52,000 individuals affected by chemical warfare [12].
Studies have revealed that the average number of chemical terrorist attacks rose from six per year to more than twenty annually between 2011 and 2017, primarily due to conflicts in Iraq and Syria [6]. The Global Terrorism Database (GTD) recorded 425 terrorist attacks involving chemical agents from 1970 to 2020, resulting in 284 fatalities and 13,267 injuries [13].
Recent research on the management of chemical terrorist incidents highlights the importance of evaluating and mitigating the psychological and social effects of such events on affected communities. One study explores the long-term psychological impact on survivors and provides recommendations for offering psychological and social support services to these individuals [14, 15].
Furthermore, other studies emphasize the critical role of regular training and drills for rescue and medical teams, which significantly enhance preparedness and efficiency in responding to chemical incidents [16, 17].
Given the increasing prevalence of chemical terrorist threats globally, the need for comprehensive and integrated studies in this area is more critical than ever. These threats pose significant risks not only to national and international security but also to public health and the environment, often causing irreparable damage. Thus, the development and implementation of integrated management strategies to address such incidents is of paramount importance. Despite numerous efforts in chemical accident management, substantial research gaps remain in this field. One major challenge is the lack of a holistic approach that addresses various aspects and stages of management during chemical terrorist incidents. Furthermore, there is a clear need for innovative and effective methods to assess and mitigate the psychological and social impacts of these incidents on affected communities. Addressing these gaps will contribute to enhancing and strengthening disaster management systems, thereby improving preparedness and response capabilities against chemical terrorist threats. Additionally, this effort will support the development of more effective strategies to combat such risks. This study aimed to identify factors related to the integrated management of chemical terrorist incidents and propose solutions to enhance emergency response efforts.
Information and Methods
This review study was conducted based on the five-step framework outlined by Arksey and O'Malley in 2024 [18].
Identification of relevant studies
This step involves the literature search process to identify articles for inclusion in the study. The research team conducted a comprehensive search of scientific databases, including PubMed, Scopus, Web of Science, Google Scholar, SID, and Magiran, for articles published between 1994 and September 2024. The search utilized relevant keywords, such as integrated management, chemical terrorism, hospital management, prehospital management, and disaster management. A combination of keywords with Boolean operators (AND/OR) was applied to refine the search strategy. For instance, the PubMed search strategy, ((((Integrated management) OR (Systems Integration) OR (incident management system)) AND ((Chemical Terrorist) OR (chemical weapons) OR (terrorism) OR (counter terrorism medicine) OR (Chemical Warfare)) AND ((Hospital management) OR (Hospital Administration) OR (Pre hospital Emergency Care) OR (Disaster Planning) OR (Disaster Management) OR (Emergency Preparedness)))), was used.
Selection of related articles
The article selection process was aligned with the research question and eligibility criteria. Two team members (SH.Z. and F.T.) independently screened the titles and abstracts during the initial stage, ensuring the removal of duplicates. Any discrepancies or conflicts were resolved through arbitration by a third member (M.A.). Following this, the research team manually reviewed the full texts of the identified articles.
The criteria for including articles in the study encompassed those that directly answered the main research question and were related to the research topic, as well as research and review articles in Persian and English. Additionally, the criteria included documents related to chemical accident management, free access to the full texts of the articles, non-repetition of content, and publication dates between 1994 and September 2024. The relevant studies were identified and agreed upon by consensus among the team.
The exclusion criteria included articles that did not address the main research question or were not directly related to the research topic, were weak in terms of methodology, or did not provide sufficient and valid data. Additionally, articles for which only abstracts were available and the full text was not accessible, as well as articles written in a language other than Persian or English—languages in which the researcher is not proficient and for which accurate translation was not feasible—were also excluded. According to the PRISMA framework, these articles were removed from the study, resulting in the selection of 14 articles for inclusion in the study (Figure 1).
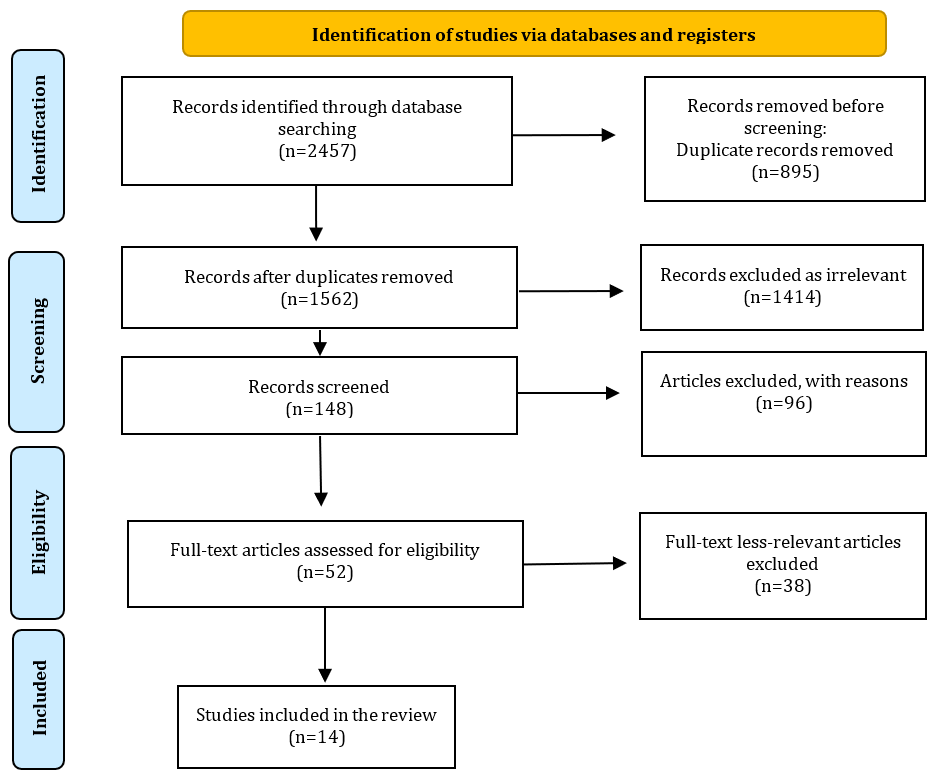
Figure 1. Study selection process guided by PRISMA.
Data analysis
Eligible articles were extracted from a data table that included parameters, such as title, author, year of publication, study location (country), study method, and findings. To ensure the effectiveness and accuracy of the data extraction process, two team members (SH.Z. and S.SH.) examined the extracted articles in detail. In cases of disagreement, a third researcher (F.T.) was consulted for assistance.
Collecting, summarizing, and reporting the results
The extracted data were summarized in a comprehensive report, identifying and discussing the important aspects of the integrated management of chemical terrorist incidents.
Findings
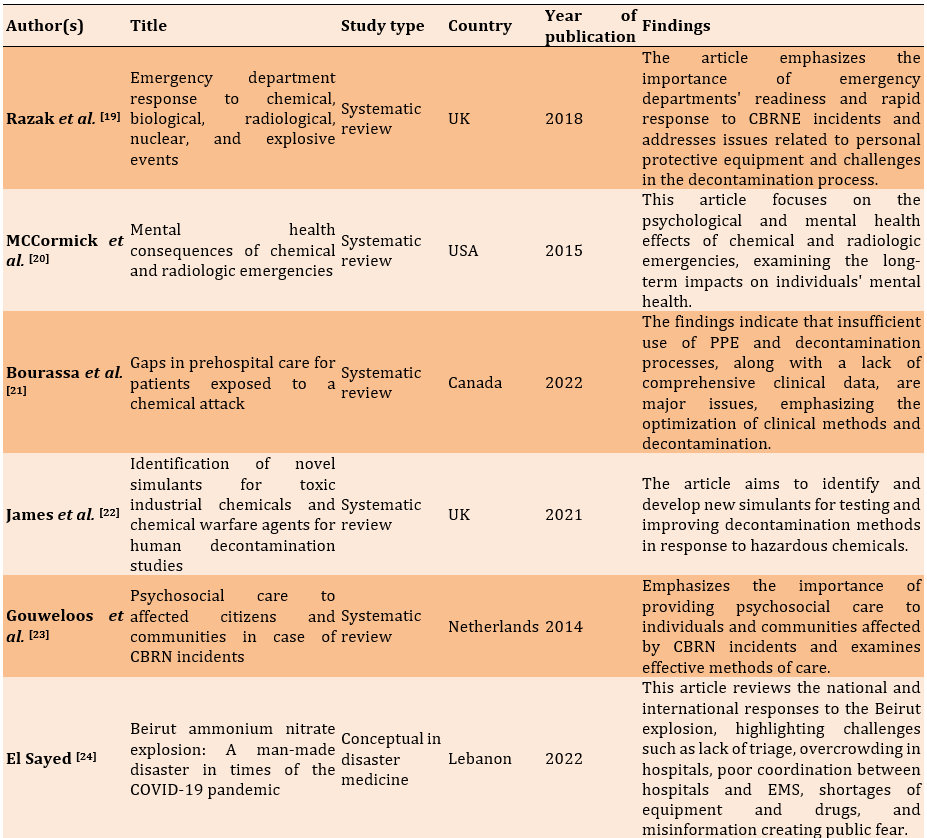
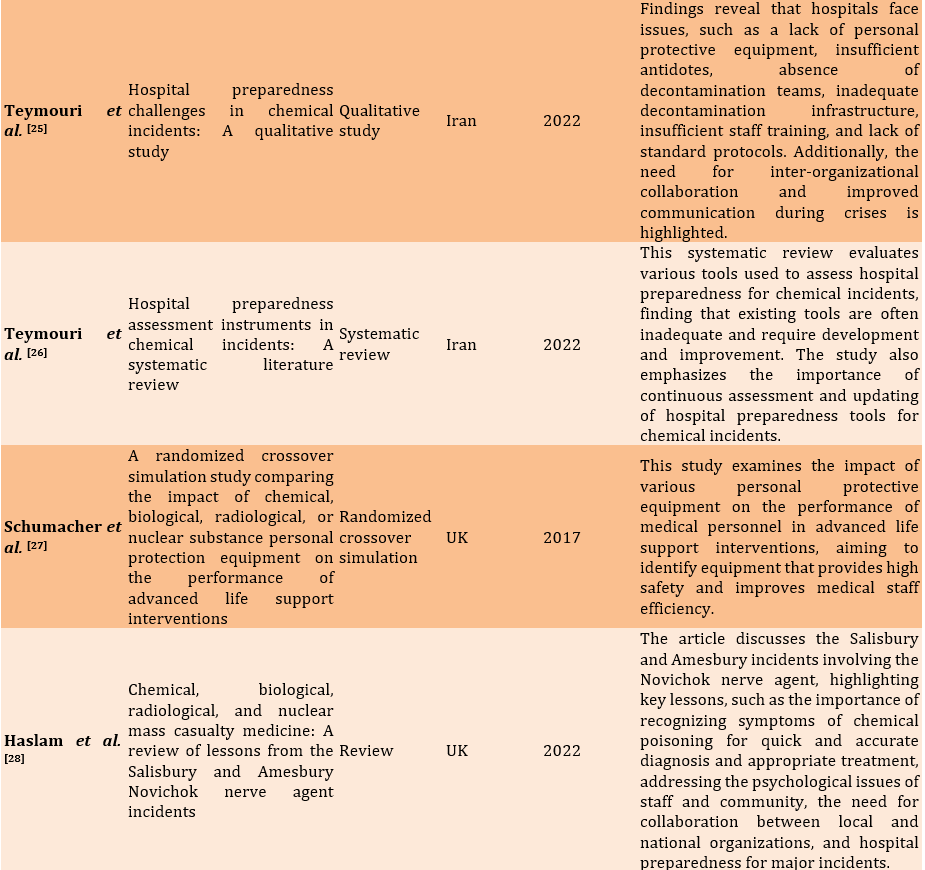
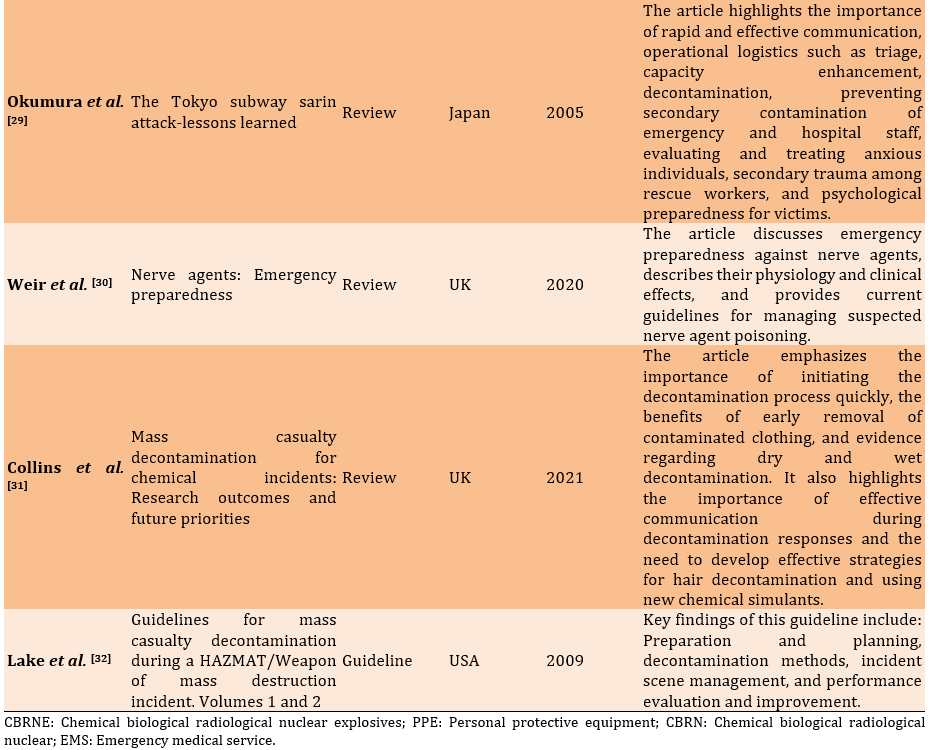
A total of 14 articles were selected for evaluation, which were conducted in England (6, 43%), Iran (2, 15%), the United States (2, 14%), Canada (1, 7%), the Netherlands (1, 7%), Japan (1, 7%), and Lebanon (1, 7%; Table 1).
Table 1. Characteristics of the studies conducted regarding the management of chemical incidents
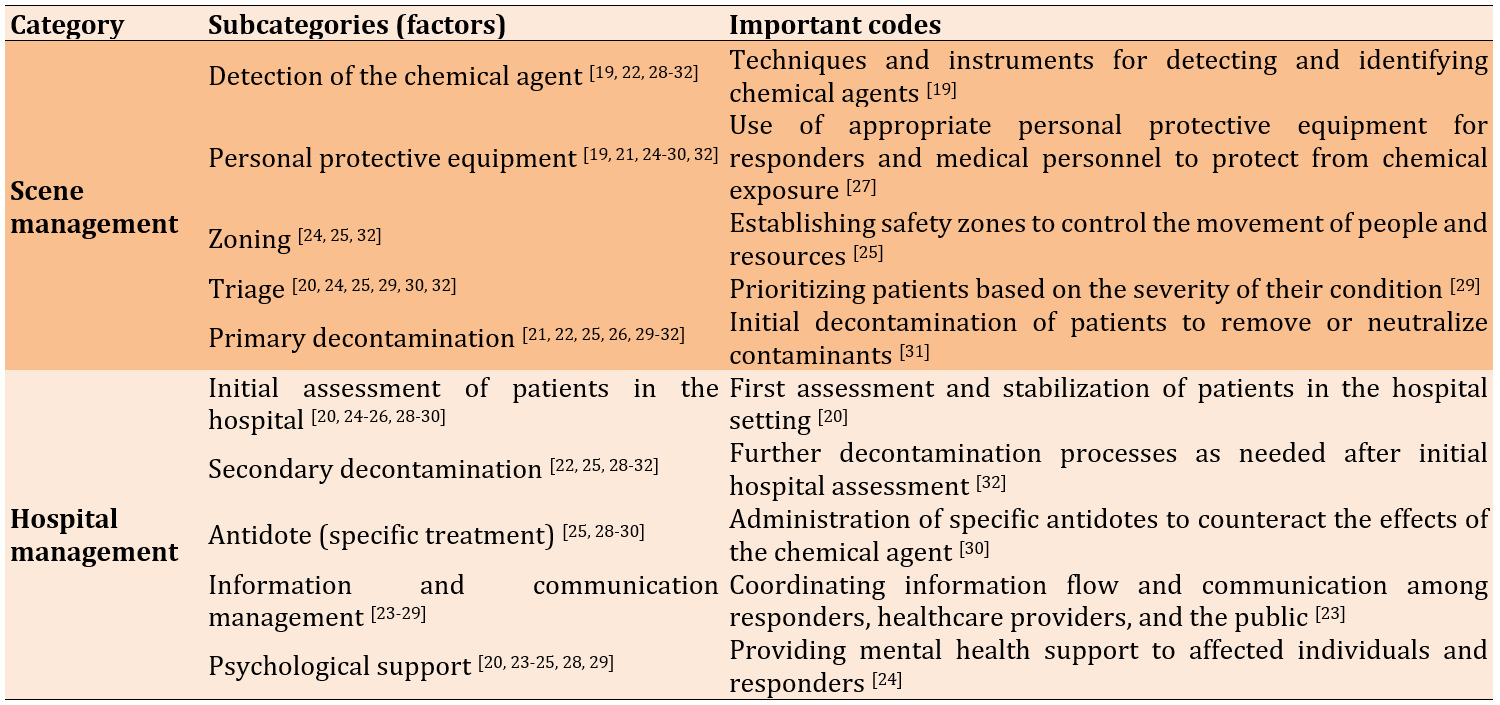
Ten identified factors related to the integrated management of chemical accidents were detection of the chemical agent, personal protective equipment, zoning, triage, primary decontamination, initial assessment of patients in the hospital, secondary decontamination, antidote (specific treatment), information and communication management, and psychological support (Table 2).
Table 2. Factors related to the integrated management of chemical terrorist incidents
Discussion
This study aimed to identify factors related to the integrated management of chemical terrorist incidents and propose solutions to enhance emergency response efforts. The initial response to a chemical terrorist incident requires a rapid and coordinated response plan. Involved agencies, including fire, police, and medical teams, must be activated immediately. The first step is to identify the type of chemical and its level of danger. Next, rescue teams must secure the area and remove people from the danger zone. These teams must be equipped with personal protective equipment. Other actions to be performed at the scene are as follows.
In response to chemical incidents, it is often necessary to initiate immediate treatment without waiting for the results of diagnostic tests. Rapid diagnosis based on clinical symptoms, physical findings, standard laboratory tests, or preliminary qualitative analyses of toxic substances, is essential. For example, in the Tokyo subway sarin gas attack, the presence of an organophosphate agent was diagnosed based on signs of parasympathetic stimulation, such as miosis, excessive nasal discharge, and low cholinesterase levels in the victims. This allowed for the timely initiation of treatment with antidotes, even before receiving laboratory results [29].
In 1998, during the Wakayama arsenic incident, it took eight days for victims to be diagnosed with arsenic poisoning, which was initially mistaken for food poisoning and later for cyanide poisoning. In response to the need for the immediate identification of chemical agents used in terrorist incidents, Japan increased its laboratory capacity and equipped 73 emergency centers across the country with advanced equipment, such as gas chromatography/mass spectrometry, high-performance liquid chromatography, and inductively coupled plasma mass spectrometry. The Japanese government also established a list of key personnel with expertise in chemical incident management, including clinical toxicologists, and created a model for coordinating responses to incidents involving the use of chemicals. Emergency responses are coordinated at the local level by an on-scene command center and at the national level by the Japan Poisons Information Center (JPIC). In this model, the EMS dispatch station collects information about the victims' condition and sends it to the JPIC. Using this information, the JPIC determines the probable cause and sends the results to the EMS dispatch center and hospitals [33].
Personal protective equipment is critical for personnel responding to chemical incidents and plays a key role in protecting them from chemical hazards. Proper selection of personal protective equipment is essential for employee safety, and specialized training for its proper use is required. According to the results of these studies, the problems associated with the use of personal protective equipment during response include the unavailability of equipment, the cumbersome nature of the gear, premature fatigue of personnel, and insufficient knowledge regarding the use of this equipment, which can lead to delays in providing critical care. However, the use of PPE is necessary to protect personnel from hazardous substances and should be accompanied by appropriate training and continuous practice to ensure that personnel can effectively and safely perform advanced supportive and therapeutic measures [27].
Prior to the 1995 sarin gas attack on the Tokyo subway, emergency response protocols for chemical incidents divided the scene into two parts; a danger (contaminated) zone and a safe (clean) zone. After that attack, the authorities recognized the importance of creating a specific physical area for the decontamination of the injured and rescue forces. Currently, based on the emergency response protocols for chemical accidents, the affected area is divided into three zones, namely the "hot" area (contaminated area), the "warm" area (where decontamination occurs), and the "cold" area (uncontaminated area). Each area serves a specific purpose in ensuring the safety of responders and casualties [33]. These three areas play important roles in the effective management of chemical accidents by ensuring the proper containment of risks, facilitating decontamination processes, and providing a safe environment for triage and medical interventions [34-36].
Triage in chemical accidents involves the rapid assessment and classification of patients based on the severity of injuries and potential exposure to hazardous chemicals. This process is critical to ensure the efficient allocation of medical resources and the timely delivery of the appropriate level of care to patients. Triage systems for chemical casualties may include color labels or other visual aids to quickly identify the level of care needed, such as red for emergency care, yellow for semi-emergency care, green for asymptomatic outpatients, and black for deceased patients. The optimal use of available resources to protect the lives of the most severely injured individuals is one of the key principles of triage [37, 38]. In the triage of chemical victims, clinical symptoms should be examined to identify the type of potential chemical substance. If there are signs of poisoning in the victim, they should be prioritized, and in cases of impaired hemodynamics, red priority should be assigned [39].
Notably, chemical accidents have the potential to cause mass casualties that require careful triage. For example, in the Japanese subway sarin gas attack, approximately 640 victims required medical and triage services [40]. Additionally, in the Beirut accident, more than 6,000 people were injured, which, due to improper triage and transfer, caused a disruption in the centers' service delivery to priority patients [24].
In the event of a chemical accident, it is necessary to remove or neutralize harmful substances from injured victims to reduce potential injuries and casualties [41]. Decontamination must be performed quickly during a chemical incident, even before the agent is identified. This is part of the immediate response and treatment [42]. The methods of decontamination may vary depending on the nature of the chemical agent used [41]. Generally, the methods of decontaminating victims are divided into two categories: "wet" (using water) and "dry" (removing clothes and using absorbent materials).
In addition to having the necessary conditions and facilities for the physical decontamination of patients, decontamination requires knowledge and management. Studies have identified several existing challenges. For example, some emergency rooms have designated areas for disinfection, but they are not equipped to manage serious chemical accidents. Additionally, there is a lack of knowledge on how to properly execute decontamination, as well as issues with managing time intervals and water flow to prevent cross-contamination. Waste management is also often not performed properly [19]. In the sarin gas attack on the Japanese subway, due to the lack of sufficient equipment and suitable spaces for decontamination, 23% of health workers suffered secondary contamination. Other methods, such as the use of swimming pools or sports centers by the government, should be considered for mass decontamination [29].
Hospital staff should be prepared to receive and treat potentially contaminated victims. The key elements of an effective hospital response plan include rapid incident identification, protection of staff and facilities, decontamination and patient triage, medical treatment, and coordination with external emergency response organizations and public health agencies [43].
After entering the hospital, the injured should be triaged again, and their condition should be evaluated, including the degree of contamination, severity of injuries, history of exposure, and presence of symptoms related to exposure. This process helps ensure the efficient allocation of resources and that the most critical patients receive care [44]. In the Beirut explosion incident, many patients were transferred to the operating room without full identification and evaluation [24]. Additionally, the presence of specialized departments for these injured individuals is important. After chemical terrorist attacks in eight major cities, Japan established NBC centers to address chemical, biological, and nuclear threats [33].
In large-scale events resulting in thousands of casualties, such as the Tokyo subway sarin attack, it would be difficult for first responders to perform thorough decontamination at the scene. As a result, these victims are transported to the hospital without decontamination or simply by having their clothes removed, which must then be decontaminated to remove any remaining chemicals from their bodies. This process is crucial for minimizing the risk of secondary contamination and preventing the spread of chemical agents within the hospital environment [45, 46]. The next step is to stabilize the condition of the injured individual in order to manage any life-threatening conditions, such as respiratory distress or cardiovascular collapse, which may require the administration of antidotes, supportive care, or other interventions [46, 47].
One of the critical aspects of responding to chemical terrorist incidents is the immediate administration of antidotes. Investigations conducted after the sarin incident in Japan have shown that, despite the need for immediate respiratory measures such as intubation, the priority is to administer antidotes. This has led to changes in rescue protocols from airway, breathing, and circulation (ABC) to antidotes, airway, breathing, and circulation (AABC), where it is emphasized that antidotes should be administered to injured individuals before any other action [29]. Chemical casualties may require supportive care, such as respiratory support, fluid resuscitation, or pain management, to address the consequences of chemical exposure [39, 40]. Additionally, in some cases, casualties may require rehabilitation services to prevent long-term effects, such as neurological or cognitive disorders [46, 47]. Therapeutic interventions may also be necessary to manage the aftermath of a chemical terrorism incident, such as distributing preventive treatments to at-risk individuals and decontaminating affected areas [48].
Proper management of information and communication is essential to reduce stress and panic symptoms [49]. The ultimate goal of information dissemination is to minimize harm to patients, healthcare providers, and the community while maximizing survival rates. The injured individuals were taken to different hospitals across the city. However, the lack of an effective system for sharing information between hospitals hindered crisis management. Initially, the cause of the accident was believed to be harmless food poisoning, but this hypothesis was rejected after the first death occurred in one of the hospitals. The hospital that witnessed the first death was unaware of the exact number of injuries in other hospitals, as well as their treatment methods, which resulted in four more deaths the following morning. Arsenic was not identified as the main cause of poisoning until eight days after the incident. Effective communication plays a key role in breaking down bureaucratic barriers and helps ensure quick and accurate decision-making, which prevents the spread of misinformation [29]. In the Beirut explosion, public information and communication remained one of the primary challenges during the response to this disaster. Problems were observed, ranging from the lack of pre-explosion notifications to the absence of official reports on response activities, such as daily updates on rescue operations, casualty identification, damage assessment, international assistance, and other recovery-related activities [24].
In terrorist incidents, the acute effects are often less severe than initially feared, while the long-term consequences can be much more complex and difficult than anticipated [23]. Previous studies have shown that the implementation of appropriate intervention strategies, such as psychological first aid, can lead to a reduction in both acute and long-term complications caused by psychological stress following disasters [20].
Recent research in the Republic of Korea has demonstrated that carefully integrating mental health considerations into post-chemical accident assessments has been effective in managing and recovering from the psychological trauma experienced by victims. This approach, which addresses both the diagnosis and treatment of psychological complications caused by contact with chemical substances, as well as psychological injuries resulting from the accident itself, has been proposed as a new standard in health responses [50].
The management of chemical terrorism incidents, from the scene to the hospital, requires preparation and coordination between prehospital and hospital management teams. Effective management of these incidents demands a coordinated effort that includes detecting the chemical agent, using personal protective equipment, establishing zoning, triage, initial decontamination, initial assessment of patients in the hospital, secondary decontamination, administering antidotes (specific treatments), managing information and communication, and providing psychological support. By understanding these key aspects, healthcare providers can better prepare for such incidents with a DMP (disaster management plan) and attention to the incident command system (ICS), ultimately saving lives and reducing the impact on affected communities.
Conclusion
Managing victims of chemical terrorist incidents requires preparation and coordination between prehospital and hospital systems.
Acknowledgments: We extend our gratitude to all the researchers whose articles were reviewed in this study.
Ethical Permissions: Not applicable.
Conflicts of Interests: The authors reported no conflicts of interests.
Authors' Contribution: Zibasokhan Sh (First Author), Introduction Writer/Main Researcher/Discussion Writer (35%); Teymouri F (Second Author), Methodologist (35%); Sharififar S (Third Author), Assistant Researcher (15%); Azizi M (Fourth Author), Assistant Researcher (15%)
Funding/Support: No financial support was received for this study.
In the modern world, due to the growing diversity of chemical production and their global application in various aspects of life, the risk of human exposure to chemicals and their associated health consequences has significantly increased [1]. Chemical accidents are recognized as serious threats [2]. The World Health Organization (WHO) defines a chemical incident as "an uncontrolled release of a toxic substance that has the potential to result in harm to public health and the environment" [3]. These incidents may occur not only as a result of industrial and domestic accidents or natural disasters but also due to intentional releases and terrorist activities [2, 4].
In recent years, threats arising from the use of chemical substances in terrorist operations have become critical security concerns at the international level. Due to their capacity to cause extensive harm, induce profound psychological effects on societies, and their relative accessibility, these materials have attracted the attention of various terrorist groups [5, 6]. Recent studies indicate a significant rise in terrorist chemical attacks over the past five decades, underscoring the need for more detailed analyses [6, 7].
The use of chemical weapons in terrorism is not a new phenomenon and has been documented throughout history. Examples date back to ancient times. In the last century, chemical agents have been employed in numerous wars [8]. The first widespread use of chemical weapons occurred during World War I when Germany utilized chlorine and mustard gas, leading to the death and injury of thousands of soldiers [9, 10].
During the Iran-Iraq War (1980–1988), there was substantial evidence of the Iraqi army’s extensive use of chemical weapons, including sulfur mustard, nerve agents, and other toxic substances [11]. Reports from the Iran-Iraq War recorded 398,587 victims among veterans, with 52,000 individuals affected by chemical warfare [12].
Studies have revealed that the average number of chemical terrorist attacks rose from six per year to more than twenty annually between 2011 and 2017, primarily due to conflicts in Iraq and Syria [6]. The Global Terrorism Database (GTD) recorded 425 terrorist attacks involving chemical agents from 1970 to 2020, resulting in 284 fatalities and 13,267 injuries [13].
Recent research on the management of chemical terrorist incidents highlights the importance of evaluating and mitigating the psychological and social effects of such events on affected communities. One study explores the long-term psychological impact on survivors and provides recommendations for offering psychological and social support services to these individuals [14, 15].
Furthermore, other studies emphasize the critical role of regular training and drills for rescue and medical teams, which significantly enhance preparedness and efficiency in responding to chemical incidents [16, 17].
Given the increasing prevalence of chemical terrorist threats globally, the need for comprehensive and integrated studies in this area is more critical than ever. These threats pose significant risks not only to national and international security but also to public health and the environment, often causing irreparable damage. Thus, the development and implementation of integrated management strategies to address such incidents is of paramount importance. Despite numerous efforts in chemical accident management, substantial research gaps remain in this field. One major challenge is the lack of a holistic approach that addresses various aspects and stages of management during chemical terrorist incidents. Furthermore, there is a clear need for innovative and effective methods to assess and mitigate the psychological and social impacts of these incidents on affected communities. Addressing these gaps will contribute to enhancing and strengthening disaster management systems, thereby improving preparedness and response capabilities against chemical terrorist threats. Additionally, this effort will support the development of more effective strategies to combat such risks. This study aimed to identify factors related to the integrated management of chemical terrorist incidents and propose solutions to enhance emergency response efforts.
Information and Methods
This review study was conducted based on the five-step framework outlined by Arksey and O'Malley in 2024 [18].
Identification of relevant studies
This step involves the literature search process to identify articles for inclusion in the study. The research team conducted a comprehensive search of scientific databases, including PubMed, Scopus, Web of Science, Google Scholar, SID, and Magiran, for articles published between 1994 and September 2024. The search utilized relevant keywords, such as integrated management, chemical terrorism, hospital management, prehospital management, and disaster management. A combination of keywords with Boolean operators (AND/OR) was applied to refine the search strategy. For instance, the PubMed search strategy, ((((Integrated management) OR (Systems Integration) OR (incident management system)) AND ((Chemical Terrorist) OR (chemical weapons) OR (terrorism) OR (counter terrorism medicine) OR (Chemical Warfare)) AND ((Hospital management) OR (Hospital Administration) OR (Pre hospital Emergency Care) OR (Disaster Planning) OR (Disaster Management) OR (Emergency Preparedness)))), was used.
Selection of related articles
The article selection process was aligned with the research question and eligibility criteria. Two team members (SH.Z. and F.T.) independently screened the titles and abstracts during the initial stage, ensuring the removal of duplicates. Any discrepancies or conflicts were resolved through arbitration by a third member (M.A.). Following this, the research team manually reviewed the full texts of the identified articles.
The criteria for including articles in the study encompassed those that directly answered the main research question and were related to the research topic, as well as research and review articles in Persian and English. Additionally, the criteria included documents related to chemical accident management, free access to the full texts of the articles, non-repetition of content, and publication dates between 1994 and September 2024. The relevant studies were identified and agreed upon by consensus among the team.
The exclusion criteria included articles that did not address the main research question or were not directly related to the research topic, were weak in terms of methodology, or did not provide sufficient and valid data. Additionally, articles for which only abstracts were available and the full text was not accessible, as well as articles written in a language other than Persian or English—languages in which the researcher is not proficient and for which accurate translation was not feasible—were also excluded. According to the PRISMA framework, these articles were removed from the study, resulting in the selection of 14 articles for inclusion in the study (Figure 1).
Figure 1. Study selection process guided by PRISMA.
Data analysis
Eligible articles were extracted from a data table that included parameters, such as title, author, year of publication, study location (country), study method, and findings. To ensure the effectiveness and accuracy of the data extraction process, two team members (SH.Z. and S.SH.) examined the extracted articles in detail. In cases of disagreement, a third researcher (F.T.) was consulted for assistance.
Collecting, summarizing, and reporting the results
The extracted data were summarized in a comprehensive report, identifying and discussing the important aspects of the integrated management of chemical terrorist incidents.
Findings
A total of 14 articles were selected for evaluation, which were conducted in England (6, 43%), Iran (2, 15%), the United States (2, 14%), Canada (1, 7%), the Netherlands (1, 7%), Japan (1, 7%), and Lebanon (1, 7%; Table 1).
Table 1. Characteristics of the studies conducted regarding the management of chemical incidents
Ten identified factors related to the integrated management of chemical accidents were detection of the chemical agent, personal protective equipment, zoning, triage, primary decontamination, initial assessment of patients in the hospital, secondary decontamination, antidote (specific treatment), information and communication management, and psychological support (Table 2).
Table 2. Factors related to the integrated management of chemical terrorist incidents
Discussion
This study aimed to identify factors related to the integrated management of chemical terrorist incidents and propose solutions to enhance emergency response efforts. The initial response to a chemical terrorist incident requires a rapid and coordinated response plan. Involved agencies, including fire, police, and medical teams, must be activated immediately. The first step is to identify the type of chemical and its level of danger. Next, rescue teams must secure the area and remove people from the danger zone. These teams must be equipped with personal protective equipment. Other actions to be performed at the scene are as follows.
In response to chemical incidents, it is often necessary to initiate immediate treatment without waiting for the results of diagnostic tests. Rapid diagnosis based on clinical symptoms, physical findings, standard laboratory tests, or preliminary qualitative analyses of toxic substances, is essential. For example, in the Tokyo subway sarin gas attack, the presence of an organophosphate agent was diagnosed based on signs of parasympathetic stimulation, such as miosis, excessive nasal discharge, and low cholinesterase levels in the victims. This allowed for the timely initiation of treatment with antidotes, even before receiving laboratory results [29].
In 1998, during the Wakayama arsenic incident, it took eight days for victims to be diagnosed with arsenic poisoning, which was initially mistaken for food poisoning and later for cyanide poisoning. In response to the need for the immediate identification of chemical agents used in terrorist incidents, Japan increased its laboratory capacity and equipped 73 emergency centers across the country with advanced equipment, such as gas chromatography/mass spectrometry, high-performance liquid chromatography, and inductively coupled plasma mass spectrometry. The Japanese government also established a list of key personnel with expertise in chemical incident management, including clinical toxicologists, and created a model for coordinating responses to incidents involving the use of chemicals. Emergency responses are coordinated at the local level by an on-scene command center and at the national level by the Japan Poisons Information Center (JPIC). In this model, the EMS dispatch station collects information about the victims' condition and sends it to the JPIC. Using this information, the JPIC determines the probable cause and sends the results to the EMS dispatch center and hospitals [33].
Personal protective equipment is critical for personnel responding to chemical incidents and plays a key role in protecting them from chemical hazards. Proper selection of personal protective equipment is essential for employee safety, and specialized training for its proper use is required. According to the results of these studies, the problems associated with the use of personal protective equipment during response include the unavailability of equipment, the cumbersome nature of the gear, premature fatigue of personnel, and insufficient knowledge regarding the use of this equipment, which can lead to delays in providing critical care. However, the use of PPE is necessary to protect personnel from hazardous substances and should be accompanied by appropriate training and continuous practice to ensure that personnel can effectively and safely perform advanced supportive and therapeutic measures [27].
Prior to the 1995 sarin gas attack on the Tokyo subway, emergency response protocols for chemical incidents divided the scene into two parts; a danger (contaminated) zone and a safe (clean) zone. After that attack, the authorities recognized the importance of creating a specific physical area for the decontamination of the injured and rescue forces. Currently, based on the emergency response protocols for chemical accidents, the affected area is divided into three zones, namely the "hot" area (contaminated area), the "warm" area (where decontamination occurs), and the "cold" area (uncontaminated area). Each area serves a specific purpose in ensuring the safety of responders and casualties [33]. These three areas play important roles in the effective management of chemical accidents by ensuring the proper containment of risks, facilitating decontamination processes, and providing a safe environment for triage and medical interventions [34-36].
Triage in chemical accidents involves the rapid assessment and classification of patients based on the severity of injuries and potential exposure to hazardous chemicals. This process is critical to ensure the efficient allocation of medical resources and the timely delivery of the appropriate level of care to patients. Triage systems for chemical casualties may include color labels or other visual aids to quickly identify the level of care needed, such as red for emergency care, yellow for semi-emergency care, green for asymptomatic outpatients, and black for deceased patients. The optimal use of available resources to protect the lives of the most severely injured individuals is one of the key principles of triage [37, 38]. In the triage of chemical victims, clinical symptoms should be examined to identify the type of potential chemical substance. If there are signs of poisoning in the victim, they should be prioritized, and in cases of impaired hemodynamics, red priority should be assigned [39].
Notably, chemical accidents have the potential to cause mass casualties that require careful triage. For example, in the Japanese subway sarin gas attack, approximately 640 victims required medical and triage services [40]. Additionally, in the Beirut accident, more than 6,000 people were injured, which, due to improper triage and transfer, caused a disruption in the centers' service delivery to priority patients [24].
In the event of a chemical accident, it is necessary to remove or neutralize harmful substances from injured victims to reduce potential injuries and casualties [41]. Decontamination must be performed quickly during a chemical incident, even before the agent is identified. This is part of the immediate response and treatment [42]. The methods of decontamination may vary depending on the nature of the chemical agent used [41]. Generally, the methods of decontaminating victims are divided into two categories: "wet" (using water) and "dry" (removing clothes and using absorbent materials).
In addition to having the necessary conditions and facilities for the physical decontamination of patients, decontamination requires knowledge and management. Studies have identified several existing challenges. For example, some emergency rooms have designated areas for disinfection, but they are not equipped to manage serious chemical accidents. Additionally, there is a lack of knowledge on how to properly execute decontamination, as well as issues with managing time intervals and water flow to prevent cross-contamination. Waste management is also often not performed properly [19]. In the sarin gas attack on the Japanese subway, due to the lack of sufficient equipment and suitable spaces for decontamination, 23% of health workers suffered secondary contamination. Other methods, such as the use of swimming pools or sports centers by the government, should be considered for mass decontamination [29].
Hospital staff should be prepared to receive and treat potentially contaminated victims. The key elements of an effective hospital response plan include rapid incident identification, protection of staff and facilities, decontamination and patient triage, medical treatment, and coordination with external emergency response organizations and public health agencies [43].
After entering the hospital, the injured should be triaged again, and their condition should be evaluated, including the degree of contamination, severity of injuries, history of exposure, and presence of symptoms related to exposure. This process helps ensure the efficient allocation of resources and that the most critical patients receive care [44]. In the Beirut explosion incident, many patients were transferred to the operating room without full identification and evaluation [24]. Additionally, the presence of specialized departments for these injured individuals is important. After chemical terrorist attacks in eight major cities, Japan established NBC centers to address chemical, biological, and nuclear threats [33].
In large-scale events resulting in thousands of casualties, such as the Tokyo subway sarin attack, it would be difficult for first responders to perform thorough decontamination at the scene. As a result, these victims are transported to the hospital without decontamination or simply by having their clothes removed, which must then be decontaminated to remove any remaining chemicals from their bodies. This process is crucial for minimizing the risk of secondary contamination and preventing the spread of chemical agents within the hospital environment [45, 46]. The next step is to stabilize the condition of the injured individual in order to manage any life-threatening conditions, such as respiratory distress or cardiovascular collapse, which may require the administration of antidotes, supportive care, or other interventions [46, 47].
One of the critical aspects of responding to chemical terrorist incidents is the immediate administration of antidotes. Investigations conducted after the sarin incident in Japan have shown that, despite the need for immediate respiratory measures such as intubation, the priority is to administer antidotes. This has led to changes in rescue protocols from airway, breathing, and circulation (ABC) to antidotes, airway, breathing, and circulation (AABC), where it is emphasized that antidotes should be administered to injured individuals before any other action [29]. Chemical casualties may require supportive care, such as respiratory support, fluid resuscitation, or pain management, to address the consequences of chemical exposure [39, 40]. Additionally, in some cases, casualties may require rehabilitation services to prevent long-term effects, such as neurological or cognitive disorders [46, 47]. Therapeutic interventions may also be necessary to manage the aftermath of a chemical terrorism incident, such as distributing preventive treatments to at-risk individuals and decontaminating affected areas [48].
Proper management of information and communication is essential to reduce stress and panic symptoms [49]. The ultimate goal of information dissemination is to minimize harm to patients, healthcare providers, and the community while maximizing survival rates. The injured individuals were taken to different hospitals across the city. However, the lack of an effective system for sharing information between hospitals hindered crisis management. Initially, the cause of the accident was believed to be harmless food poisoning, but this hypothesis was rejected after the first death occurred in one of the hospitals. The hospital that witnessed the first death was unaware of the exact number of injuries in other hospitals, as well as their treatment methods, which resulted in four more deaths the following morning. Arsenic was not identified as the main cause of poisoning until eight days after the incident. Effective communication plays a key role in breaking down bureaucratic barriers and helps ensure quick and accurate decision-making, which prevents the spread of misinformation [29]. In the Beirut explosion, public information and communication remained one of the primary challenges during the response to this disaster. Problems were observed, ranging from the lack of pre-explosion notifications to the absence of official reports on response activities, such as daily updates on rescue operations, casualty identification, damage assessment, international assistance, and other recovery-related activities [24].
In terrorist incidents, the acute effects are often less severe than initially feared, while the long-term consequences can be much more complex and difficult than anticipated [23]. Previous studies have shown that the implementation of appropriate intervention strategies, such as psychological first aid, can lead to a reduction in both acute and long-term complications caused by psychological stress following disasters [20].
Recent research in the Republic of Korea has demonstrated that carefully integrating mental health considerations into post-chemical accident assessments has been effective in managing and recovering from the psychological trauma experienced by victims. This approach, which addresses both the diagnosis and treatment of psychological complications caused by contact with chemical substances, as well as psychological injuries resulting from the accident itself, has been proposed as a new standard in health responses [50].
The management of chemical terrorism incidents, from the scene to the hospital, requires preparation and coordination between prehospital and hospital management teams. Effective management of these incidents demands a coordinated effort that includes detecting the chemical agent, using personal protective equipment, establishing zoning, triage, initial decontamination, initial assessment of patients in the hospital, secondary decontamination, administering antidotes (specific treatments), managing information and communication, and providing psychological support. By understanding these key aspects, healthcare providers can better prepare for such incidents with a DMP (disaster management plan) and attention to the incident command system (ICS), ultimately saving lives and reducing the impact on affected communities.
Conclusion
Managing victims of chemical terrorist incidents requires preparation and coordination between prehospital and hospital systems.
Acknowledgments: We extend our gratitude to all the researchers whose articles were reviewed in this study.
Ethical Permissions: Not applicable.
Conflicts of Interests: The authors reported no conflicts of interests.
Authors' Contribution: Zibasokhan Sh (First Author), Introduction Writer/Main Researcher/Discussion Writer (35%); Teymouri F (Second Author), Methodologist (35%); Sharififar S (Third Author), Assistant Researcher (15%); Azizi M (Fourth Author), Assistant Researcher (15%)
Funding/Support: No financial support was received for this study.
Keywords:
References
1. Naidu R, Biswas B, Willett IR, Cribb J, Kumar Singh B, Paul Nathanail C, et al. Chemical pollution: A growing peril and potential catastrophic risk to humanity. Environ Int. 2021;156:106616. [Link] [DOI:10.1016/j.envint.2021.106616]
2. Gaulton T, Hague C, Cole D, Thomas E, Duarte-Davidson R. Global event-based surveillance of chemical incidents. J Expo Sci Environ Epidemiol. 2023;33(1):111-7. [Link] [DOI:10.1038/s41370-021-00384-8]
3. WHO. Chemical incidents [Internet]. Geneva: World Health Organization [cited 2025, 01, 07]. Available from: https://www.who.int/health-topics/chemical-incidents#tab=tab_1. [Link]
4. Nelms D, Bernat E. Key findings: Chemical incident tracking 2021-2023. Brattleboro: Coming Clean, Inc; 2023. [Link]
5. Mills DS. Building environmental public health framework for chemical emergencies. J Environ Health. 2014;77(3):32-3. [Link]
6. DeLuca MA, Chai PR, Goralnick E, Erickson TB. Five decades of global chemical terror attacks: Data analysis to inform training and preparedness. Disaster Med Public Health Prep. 2021;15(6):750-61. [Link] [DOI:10.1017/dmp.2020.176]
7. Gonciarz A, Pich R. Increased risk of chemical terror attacks. Sci Rep Fire Univ. 2024;2(89):109-26. [Link] [DOI:10.5604/01.3001.0054.3831]
8. Lee EC. Clinical manifestations of sarin nerve gas exposure. JAMA. 2003;290(5):659-62. [Link] [DOI:10.1001/jama.290.5.659]
9. Fitzgerald GJ. Chemical warfare and medical response during World War I. Am J Public Health. 2008;98(4):611-25. [Link] [DOI:10.2105/AJPH.2007.111930]
10. Szinicz L. History of chemical and biological warfare agents. Toxicology. 2005;214(3):167-81. [Link] [DOI:10.1016/j.tox.2005.06.011]
11. Amini H, Solaymani-Dodaran M, Mousavi B, Alam Beladi SN, Soroush MR, Abolghasemi J, et al. Long-term health outcomes among survivors exposed to sulfur mustard in Iran. JAMA Netw Open. 2020;3(12):e2028894. [Link] [DOI:10.1001/jamanetworkopen.2020.28894]
12. Salamati P, Razavi SM, Shokraneh F, Mohazzab Torabi S, Laal M, Hadjati G, et al. Mortality and injuries among Iranians in Iraq-Iran war: A systematic review. Arch Iran Med. 2013;16(9):542-50. [Link]
13. Tin D, Ciottone GR. Chemical agent use in terrorist events: A gathering storm requiring enhanced civilian preparedness. Prehosp Disaster Med. 2022;37(3):327-32. [Link] [DOI:10.1017/S1049023X22000528]
14. Masoumbeigi H, Ghanizadeh G. Principles and requirements of prevention and management of chemical poisoning incidents in educational institutions: A narrative review. J Mil Med. 2023;25(3):1850-60. [Persian] [Link]
15. Barnes G, Baxter J, Litva A, Staples B. The social and psychological impact of the chemical contamination incident in Weston Village, UK: A qualitative analysis. Soc Sci Med. 2002;55(12):2227-41. [Link] [DOI:10.1016/S0277-9536(01)00367-7]
16. Balali-Mood M, Mateos R, Pita R, Rhys P, Romano J, Tirman H, et al. Practical guide for medical management of chemical warfare casualties. Netherlands: Organisation for the Prohibition of Chemical Weapons; 2016. [Persian] [Link]
17. Yu ZF, Guan JL. Fire and rescue combat technical training system construction for dangerous chemicals. Procedia Eng. 2016;135:655-60. [Link] [DOI:10.1016/j.proeng.2016.01.133]
18. Arksey H, O'Malley L. Scoping studies: Towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19-32. [Link] [DOI:10.1080/1364557032000119616]
19. Razak S, Hignett S, Barnes J. Emergency department response to chemical, biological, radiological, nuclear, and explosive events: A systematic review. Prehosp Disaster Med. 2018;33(5):543-9. [Link] [DOI:10.1017/S1049023X18000900]
20. MCCormick LC, Tajeu GS, Klapow J. Mental health consequences of chemical and radiologic emergencies: A systematic review. Emerg Med Clin North Am. 2015;33(1):197-211. [Link] [DOI:10.1016/j.emc.2014.09.012]
21. Bourassa S, Paquette-Raynard E, Noebert D, Dauphin M, Akinola PS, Marseilles J, et al. Gaps in prehospital care for patients exposed to a chemical attack-A systematic review. Prehosp Disaster Med. 2022;37(2):1-10. [Link] [DOI:10.1017/S1049023X22000401]
22. James T, Collins S, Marczylo T. Identification of novel simulants for toxic industrial chemicals and chemical warfare agents for human decontamination studies: A systematic review and categorisation of physicochemical characteristics. Int J Environ Res Public Health. 2021;18(16):8681. [Link] [DOI:10.3390/ijerph18168681]
23. Gouweloos J, Dückers M, Te Brake H, Kleber R, Drogendijk A. Psychosocial care to affected citizens and communities in case of CBRN incidents: A systematic review. Environ Int. 2014;72:46-65. [Link] [DOI:10.1016/j.envint.2014.02.009]
24. El Sayed MJ. Beirut ammonium nitrate explosion: A man-made disaster in times of the COVID-19 pandemic. Disaster Med Public Health Prep. 2022;16(3):1203-7. [Link] [DOI:10.1017/dmp.2020.451]
25. Teymouri F, Zareiyan A, Pishgooie AM, Bagheri H. Hospital preparedness challenges in chemical incidents: A qualitative study. Iran J War Public Health. 2022;14(4):377-84. [Link]
26. Teymouri F, Zareiyan A, Pishgooie AM, Bagheri H. Hospital preparedness assessment instruments in chemical incidents: A systematic literature review. Asia Pac J Health Manag. 2022;17(3):160-72. [Link] [DOI:10.24083/apjhm.v17i3.1779]
27. Schumacher J, Arlidge J, Garnham F, Ahmad I. A randomised crossover simulation study comparing the impact of chemical, biological, radiological or nuclear substance personal protection equipment on the performance of advanced life support interventions. Anaesthesia. 2017;72(5):592-7. [Link] [DOI:10.1111/anae.13842]
28. Haslam JD, Russell P, Hill S, Emmett SR, Blain PG. Chemical, biological, radiological, and nuclear mass casualty medicine: A review of lessons from the Salisbury and Amesbury Novichok nerve agent incidents. Br J Anaesth. 2022;128(2):e200-5. [Link] [DOI:10.1016/j.bja.2021.10.008]
29. Okumura T, Hisaoka T, Yamada A, Naito T, Isonuma H, Okumura S, et al. The Tokyo subway sarin attack-lessons learned. Toxicol Appl Pharmacol. 2005;207(2 Suppl):471-6. [Link] [DOI:10.1016/j.taap.2005.02.032]
30. Weir AGA, Makin S, Breeze J. Nerve agents: Emergency preparedness. BMJ Mil Health. 2020;166(1):42-6. [Link] [DOI:10.1136/jramc-2019-001380]
31. Collins S, James T, Carter H, Symons C, Southworth F, Foxall K, et al. Mass casualty decontamination for chemical incidents: Research outcomes and future priorities. Int J Environ Res Public Health. 2021;18(6):3079. [Link] [DOI:10.3390/ijerph18063079]
32. Lake W, Schulze P, Gougelet R. Guidelines for mass casualty decontamination during a HAZMAT/Weapon of mass destruction incident. Volumes 1 and 2. Maryland: Edgewood Chemical Biological Center; 2009. [Link] [DOI:10.21236/ADA498442]
33. Okumura T, Ninomiya N, Ohta M. The chemical disaster response system in Japan. Prehosp Disaster Med. 2003;18(3):189-92. [Link] [DOI:10.1017/S1049023X00001047]
34. Kenar L, Karayilanoglu T. Prehospital management and medical intervention after a chemical attack. Emerg Med J. 2004;21(1):84-8. [Link] [DOI:10.1136/emj.2003.005488]
35. EPA. Safety zones [Internet]. Washington DC: United States Environmental Protection Agency; 2023 [cited 2024, 09, 30]. Available from: https://www.epa.gov/emergency-response/safety-zones. [Link]
36. FEMA. Site localization of decontamination [Internet]. Hyattsville: Federal Emergency Management Agency; 2023 [cited 2022, 10, 22]. Available from: https://www.fema.gov/cbrn-tools/key-planning-factors-chemical-incident/kpf4/3/3-4. [Link]
37. Bazyar J, Farrokhi M, Salari A, Khankeh HR. The principles of triage in emergencies and disasters: A systematic review. Prehosp Disaster Med. 2020;35(3):305-13. [Link] [DOI:10.1017/S1049023X20000291]
38. Teymouri F, Seyedi R, Pishgooie AH, Seyedi R. The effect of multimedia training on the attitude of military nurses in the triage of chemical casualties. J Mil Med. 2024;26(2):2269-76. [Persian] [Link]
39. Khoshnevis MA, Panahi Y, Ghanei M, Borna H, Sahebkar A, Aslani J. A triage model for chemical warfare casualties. Trauma Mon. 2015;20(3):e16211. [Link] [DOI:10.5812/traumamon.16211]
40. Okumura T, Takasu N, Ishimatsu S, Miyanoki S, Mitsuhashi A, Kumada K, et al. Report on 640 victims of the Tokyo subway sarin attack. Ann Emerg Med. 1996;28(2):129-35. [Link] [DOI:10.1016/S0196-0644(96)70052-5]
41. James T, Wyke S, Marczylo T, Collins S, Gaulton T, Foxall K, et al. Chemical warfare agent simulants for human volunteer trials of emergency decontamination: A systematic review. J Appl Toxicol. 2018;38(1):113-21. [Link] [DOI:10.1002/jat.3527]
42. Ramesh AC, Kumar S. Triage, monitoring, and treatment of mass casualty events involving chemical, biological, radiological, or nuclear agents. J Pharm Bioallied Sci. 2010;2(3):239-47. [Link] [DOI:10.4103/0975-7406.68506]
43. Georgopoulos PG, Fedele P, Shade P, Lioy PJ, Hodgson M, Longmire A, et al. Hospital response to chemical terrorism: Personal protective equipment, training, and operations planning. Am J Ind Med. 2004;46(5):432-45. [Link] [DOI:10.1002/ajim.20075]
44. Cone DC, Koenig KL. Mass casualty triage in the chemical, biological, radiological, or nuclear environment. Eur J Emerg Med. 2005;12(6):287-302. [Link] [DOI:10.1097/00063110-200512000-00009]
45. Anan H, Otomo Y, Homma M, Oshiro K, Kondo H, Shimamura F, et al. Proposal for reforming prehospital response to chemical terrorism disasters in Japan: Going back to the basics of saving the lives of the injured by securing the safety of the rescue team. Prehosp Disaster Med. 2020;35(1):88-91. [Link] [DOI:10.1017/S1049023X19005119]
46. Jiang Y. Analysis of the toxicity and treatment methods of cyanide. Theor Nat Sci. 2023;27(1):235-40. [Link] [DOI:10.54254/2753-8818/27/20240741]
47. Tadmor B, Marcus N, Givoni S, Winder A. Prevention and management of chemical and biological casualties. Prehospital Dis Med. 1999;14(Suppl S1):S63-4. [Link] [DOI:10.1017/S1049023X0003421X]
48. Casillas RP, Tewari-Singh N, Gray JP. Special issue: Emerging chemical terrorism threats. Toxicol Mech Methods. 2021;31(4):239-41. [Link] [DOI:10.1080/15376516.2021.1904472]
49. Tan ATH. A review of: "Hall Gardner. American global strategy and the "war on terrorism"". Terror Polit Violence. 2010;22(2):317-8. [Link] [DOI:10.1080/09546551003617960]
50. WHO. Case study: Managing the public health impact of chemical incidents in the Republic of Korea. Geneva: World Health Organization; 2023. [Link]