
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

1.0
Cite Score 2025
SJR: 0.129 / SNIP: 0.140
Volume 13, Issue 2 (2021)
Iran J War Public Health 2021, 13(2): 103-108 |
Back to browse issues page
Article Type:
Subject:




History
Received: 2021/08/12 | Accepted: 2021/08/30 | Published: 2021/09/28
Received: 2021/08/12 | Accepted: 2021/08/30 | Published: 2021/09/28
How to cite this article
Afshani S, Shiri-Mohammadabad H, Hosseini-Motlagh S. Relationship of Health Literacy and Lifestyle in Veterans and Non-Veterans Families. Iran J War Public Health 2021; 13 (2) :103-108
URL: http://ijwph.ir/article-1-990-en.html
URL: http://ijwph.ir/article-1-990-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Department of Cooperative and Social Welfare, Faculty of Social science, Yazd University, Yazd, Iran , afshanialireza@yazd.ac.ir
2- Department of Cooperative and Social Welfare, Faculty of Social science, Yazd University, Yazd, Iran
3- Janbazan Medical and Engineering Research Center, Tehran, Iran
2- Department of Cooperative and Social Welfare, Faculty of Social science, Yazd University, Yazd, Iran
3- Janbazan Medical and Engineering Research Center, Tehran, Iran
Full-Text (HTML) (1099 Views)
Introduction
Iraq's eight-year-long war against Iran caused many damages to the country. Many deaths, injuries, and losses of the best people [1]. The war also had wide consequences, such as many physical and psychological problems and indirect effects on their families. Because the family members of a veteran, as the main agents in the care of the veteran, suffer from many psychological problems [2], it is necessary to be realistic about the problems of the veterans and their families.
One factor that can affect the resilience and health of the veterans and their families is their lifestyle. Lifestyle refers to health-related behavioral patterns that can prevent health-related problems and largely ensure one's health [3]. An important principle in health-related behaviors that make up an individual's lifestyle is their participation and admittance of responsibility to prevent infirmity and complication by performing proper health-related behaviors [4] and have a healthy lifestyle. Lifestyle is a multidimensional and complex construct determined by the individual's assessment of their situation in terms of certain conditions such as physical, mental, and social states [5]. Existing literature on the lifestyle of veterans indicates that several social factors can affect this multidimensional construct, one of which is health literacy.
Health literacy was introduced as a defining factor in reducing inequalities related to health in the United States in the mid-1970s [6, 7]. It was then considered an individual's capacity to obtain, process, and understand the basic health information and services needed to make appropriate health care decisions [8]. Health literacy is a set of skills and abilities in various ways: skills and abilities in the acquisition and access of medical and health information, skills and abilities in understanding such information, skills and abilities in processing and interpretation of the information, and skills and abilities in decision-making and use of updated information [9]. Therefore, it is necessary to measure health literacy, special design interventions to increase it, and avoid the possibility of risks due to limited literacy, especially among vulnerable groups such as veterans and their families.
Many studies show the effective role of health literacy in promoting lifestyle. Klinker et al. [10], Kudo et al. [11], Wang et al. [12], and Shieh & Halstead [13] indicated that health literacy plays an important role in promoting the health of individuals to lead a healthy lifestyle because the quality of life is affected by a good social, mental and healthy life. Providing proper information and improving health literacy in people can help improve their quality of Lifestyle [14].
Given that war has many different consequences for people, and these consequences have several effects depending on the duration of the war, its severity, and extent, people who fought in the war for their borders and lands, have received physical and mental disabilities resulting in aftermath problems of quality of life and lifestyle for them and those around them [15]. It is thus important to pay attention to the lifestyle of the veterans and their families. This study aimed to investigate the correlation between health literacy and the lifestyle of veterans and non-veterans and their families to examine the difference between the lifestyle of these families.
Instrument and Methods
A descriptive cross-sectional survey was conducted on veteran and non-veteran populations across Iran In 2019. The Deputy of Management and Human Resources Development of the Ministry of Interior of Iran has divided the provinces of Iran into five large regions based on characteristics such as proximity, geographical location, and commonalities. They are Region 1: Provinces of Tehran, Qazvin, Mazandaran, Semnan, Golestan, Alborz, and Qom; Region 2: Isfahan, Fars, Bushehr, Chaharmahal Bakhtiari, Hormozgan, Kohkiluyeh, and Boyer-Ahmad provinces; 3: Provinces of East Azerbaijan, West Azerbaijan, Ardabil, Zanjan, Gilan and Kurdistan; Region 4: Provinces of Kermanshah, Ilam, Lorestan, Hamedan, Markazi and Khuzestan, and Region 5: Provinces of Khorasan Razavi, South Khorasan, North Khorasan, Kerman, Yazd and Sistan and Baluchestan [16]. Because it was not possible to conduct the study in all the provinces (financial requirements, facilities, etc.), it was decided to select one province from each region: From Region 1: Tehran Province, Region 2: Isfahan Province, Region 3: Gilan Province, Region 4: Ilam Province, and Region 5: Khorasan Razavi Province. Due to the large size of the statistical population in each province, each province's center was considered the largest and most important city in the province for the study.
SPSS Sample Power software was used to estimate the sample size. The sample size for the veteran group was 600 and for the non-veteran group was 1200 with a total of 1800 people to meet the purpose of the research and the assumptions related to testing the hypothesis (Error Type I maximum 0.05, error Type II maximum 0.20, and the volume of the effect showing the minimum difference of 0.5 in the range of 1 to 5 between the two groups). In total, 120 veterans and 240 non-veterans were selected in each province. Therefore, in the five studied provinces, 600 veterans and 1,200 non-veterans were selected. After removing the carelessly completed responses, 1770 questionnaires were analyzed. The sampling method was such that to select the samples; first, the list of veterans and the exact address of the residence was obtained from Martyr Foundation and Veterans Affairs. Then, 120 addresses were randomly selected as veteran samples, and the researcher went to their home and completed the questionnaire. If he were not at home at the moment, he would be referred two more times, and if, after three visits, he failed to be interviewed or, for some reason, refused to be interviewed, another address would be replaced from the list of veterans. After the completion of the questionnaire by the veteran, two neighboring homes to the veteran's home were selected as non-veteran samples (The reason for choosing adjacent homes was to eliminate the effect of variables such as residence and social class that can affect lifestyle). If the non-veteran were not present or refused to be interviewed, the adjacent home would be replaced by another home. Inclusion criteria were being Iranian, over 15, having no severe mental disorders such as acute psychosis, severe mental problems such as dementia and delirium, or problems such as deafness (based on self-reported responses or surveyor's observations).
The research instruments included the following standard questionnaires:
- Lifestyle Questionnaire (LSQ) [17]: This questionnaire, designed in 2012, includes 70 items and ten components. Each item has four options: "Always" with a score of 3, "Usually" with a score of 2, "Sometimes" with a score of 1, and "Never" with a score of 0. Higher scores indicate a healthy lifestyle. A total score of 210 indicates a healthy lifestyle, and a total score of 0 indicates an unhealthy lifestyle. The questionnaire had been validated by Lali et al. through content validity calculation, factor analysis, and convergent validity computation methods [17]. Cronbach's alpha and test-retest with a 6-week interval were used on a group of 60 people to obtain the instrument's reliability [17]. This instrument has been used in several other studies [18, 19].
- All Aspects of Health Literacy Scale (AAHLS) [20]: This questionnaire was designed by Chinn and McCarthy in 2013. It consists of 13 items and three subscales, including functional health literacy, critical health literacy, and communicative health literacy. The questions of each scale are listed in the sequence in that questions 1 to 3 are related to the functional health literacy subscale, questions 4 to 9 are related to the critical health literacy subscale, and questions 10 to 13 are related to the communicative health literacy subscale. The reliability of this scale was reported by Chinn and McCarthy to be 0.74 [20].
The research was approved by the University/Regional Research Ethics Committee Veterans and martyr’s affair foundation (VMFA). Informed consent was obtained from all participants. All methods were performed in accordance with the relevant guidelines and regulations of Declaration of Helsinki. Questionnaires were completed between 9 am to 6 pm at the respondent's place of residence. The trust of the respondents was gained by presenting an ID card and a letter of introduction as well as sufficient explanations.
Independent t-test was used to compare the lifestyles of veteran and non-veteran men and women in the provinces. Also, Pearson correlation test was used to examine the relationship between the life style and health literacy. All analyses were conducted using SPSS 24.
Findings
Out of 1770 participants, the majority of them were women (58.6%), and the rest were men (41.4%). People had an age range of 15-89 years, and the mean±SD age in each province was as follows: (Gilan=51.09±18.85; Ilam=35.66±13.31; Khorasan Razavi=39.39±16.09; Tehran=44.14±15.39; Isfahan=45.17±19.04). In terms of education, most of these people had diploma degrees (32.1%).
There was no significant difference between the mean scores of the lifestyle in the two groups of veterans and non-veterans in all five provinces studied (p<0.05). Overall, the mean±SD scores of the lifestyle in the male veteran group were higher than the non-veteran group (p<0.05), although the difference between the means was small and was only significant for the large sample size (Table 1).
Also, there was no significant difference between the mean lifestyle scores in the two groups of female veterans and non-veterans in all five provinces studied except Tehran and Ilam (p<0.05). However, the difference between the means was small, and the significance was only due to the large sample size. In general, there was no significant difference between the mean scores of the lifestyle in the two groups of female veterans and female non-veterans (p<0.05) (Table 1).
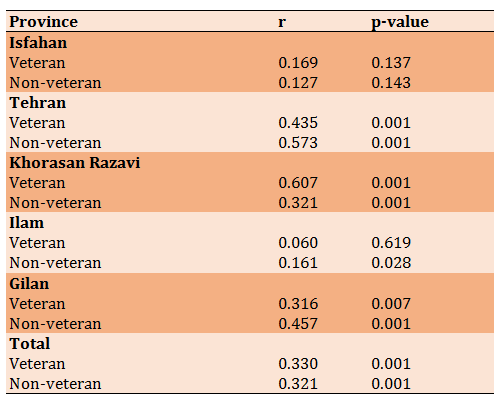
There was a direct and significant relationship between health literacy of veterans and non-veterans and their lifestyle (p<0.001). The output of this test was significant in Tehran, Khorasan Razavi, and Gilan provinces (Table 2). Also, the results of the relationship between participants' health literacy and their lifestyle in Ilam province indicate that this relationship was significant only in the non-veteran group (p<0.05).
Iraq's eight-year-long war against Iran caused many damages to the country. Many deaths, injuries, and losses of the best people [1]. The war also had wide consequences, such as many physical and psychological problems and indirect effects on their families. Because the family members of a veteran, as the main agents in the care of the veteran, suffer from many psychological problems [2], it is necessary to be realistic about the problems of the veterans and their families.
One factor that can affect the resilience and health of the veterans and their families is their lifestyle. Lifestyle refers to health-related behavioral patterns that can prevent health-related problems and largely ensure one's health [3]. An important principle in health-related behaviors that make up an individual's lifestyle is their participation and admittance of responsibility to prevent infirmity and complication by performing proper health-related behaviors [4] and have a healthy lifestyle. Lifestyle is a multidimensional and complex construct determined by the individual's assessment of their situation in terms of certain conditions such as physical, mental, and social states [5]. Existing literature on the lifestyle of veterans indicates that several social factors can affect this multidimensional construct, one of which is health literacy.
Health literacy was introduced as a defining factor in reducing inequalities related to health in the United States in the mid-1970s [6, 7]. It was then considered an individual's capacity to obtain, process, and understand the basic health information and services needed to make appropriate health care decisions [8]. Health literacy is a set of skills and abilities in various ways: skills and abilities in the acquisition and access of medical and health information, skills and abilities in understanding such information, skills and abilities in processing and interpretation of the information, and skills and abilities in decision-making and use of updated information [9]. Therefore, it is necessary to measure health literacy, special design interventions to increase it, and avoid the possibility of risks due to limited literacy, especially among vulnerable groups such as veterans and their families.
Many studies show the effective role of health literacy in promoting lifestyle. Klinker et al. [10], Kudo et al. [11], Wang et al. [12], and Shieh & Halstead [13] indicated that health literacy plays an important role in promoting the health of individuals to lead a healthy lifestyle because the quality of life is affected by a good social, mental and healthy life. Providing proper information and improving health literacy in people can help improve their quality of Lifestyle [14].
Given that war has many different consequences for people, and these consequences have several effects depending on the duration of the war, its severity, and extent, people who fought in the war for their borders and lands, have received physical and mental disabilities resulting in aftermath problems of quality of life and lifestyle for them and those around them [15]. It is thus important to pay attention to the lifestyle of the veterans and their families. This study aimed to investigate the correlation between health literacy and the lifestyle of veterans and non-veterans and their families to examine the difference between the lifestyle of these families.
Instrument and Methods
A descriptive cross-sectional survey was conducted on veteran and non-veteran populations across Iran In 2019. The Deputy of Management and Human Resources Development of the Ministry of Interior of Iran has divided the provinces of Iran into five large regions based on characteristics such as proximity, geographical location, and commonalities. They are Region 1: Provinces of Tehran, Qazvin, Mazandaran, Semnan, Golestan, Alborz, and Qom; Region 2: Isfahan, Fars, Bushehr, Chaharmahal Bakhtiari, Hormozgan, Kohkiluyeh, and Boyer-Ahmad provinces; 3: Provinces of East Azerbaijan, West Azerbaijan, Ardabil, Zanjan, Gilan and Kurdistan; Region 4: Provinces of Kermanshah, Ilam, Lorestan, Hamedan, Markazi and Khuzestan, and Region 5: Provinces of Khorasan Razavi, South Khorasan, North Khorasan, Kerman, Yazd and Sistan and Baluchestan [16]. Because it was not possible to conduct the study in all the provinces (financial requirements, facilities, etc.), it was decided to select one province from each region: From Region 1: Tehran Province, Region 2: Isfahan Province, Region 3: Gilan Province, Region 4: Ilam Province, and Region 5: Khorasan Razavi Province. Due to the large size of the statistical population in each province, each province's center was considered the largest and most important city in the province for the study.
SPSS Sample Power software was used to estimate the sample size. The sample size for the veteran group was 600 and for the non-veteran group was 1200 with a total of 1800 people to meet the purpose of the research and the assumptions related to testing the hypothesis (Error Type I maximum 0.05, error Type II maximum 0.20, and the volume of the effect showing the minimum difference of 0.5 in the range of 1 to 5 between the two groups). In total, 120 veterans and 240 non-veterans were selected in each province. Therefore, in the five studied provinces, 600 veterans and 1,200 non-veterans were selected. After removing the carelessly completed responses, 1770 questionnaires were analyzed. The sampling method was such that to select the samples; first, the list of veterans and the exact address of the residence was obtained from Martyr Foundation and Veterans Affairs. Then, 120 addresses were randomly selected as veteran samples, and the researcher went to their home and completed the questionnaire. If he were not at home at the moment, he would be referred two more times, and if, after three visits, he failed to be interviewed or, for some reason, refused to be interviewed, another address would be replaced from the list of veterans. After the completion of the questionnaire by the veteran, two neighboring homes to the veteran's home were selected as non-veteran samples (The reason for choosing adjacent homes was to eliminate the effect of variables such as residence and social class that can affect lifestyle). If the non-veteran were not present or refused to be interviewed, the adjacent home would be replaced by another home. Inclusion criteria were being Iranian, over 15, having no severe mental disorders such as acute psychosis, severe mental problems such as dementia and delirium, or problems such as deafness (based on self-reported responses or surveyor's observations).
The research instruments included the following standard questionnaires:
- Lifestyle Questionnaire (LSQ) [17]: This questionnaire, designed in 2012, includes 70 items and ten components. Each item has four options: "Always" with a score of 3, "Usually" with a score of 2, "Sometimes" with a score of 1, and "Never" with a score of 0. Higher scores indicate a healthy lifestyle. A total score of 210 indicates a healthy lifestyle, and a total score of 0 indicates an unhealthy lifestyle. The questionnaire had been validated by Lali et al. through content validity calculation, factor analysis, and convergent validity computation methods [17]. Cronbach's alpha and test-retest with a 6-week interval were used on a group of 60 people to obtain the instrument's reliability [17]. This instrument has been used in several other studies [18, 19].
- All Aspects of Health Literacy Scale (AAHLS) [20]: This questionnaire was designed by Chinn and McCarthy in 2013. It consists of 13 items and three subscales, including functional health literacy, critical health literacy, and communicative health literacy. The questions of each scale are listed in the sequence in that questions 1 to 3 are related to the functional health literacy subscale, questions 4 to 9 are related to the critical health literacy subscale, and questions 10 to 13 are related to the communicative health literacy subscale. The reliability of this scale was reported by Chinn and McCarthy to be 0.74 [20].
The research was approved by the University/Regional Research Ethics Committee Veterans and martyr’s affair foundation (VMFA). Informed consent was obtained from all participants. All methods were performed in accordance with the relevant guidelines and regulations of Declaration of Helsinki. Questionnaires were completed between 9 am to 6 pm at the respondent's place of residence. The trust of the respondents was gained by presenting an ID card and a letter of introduction as well as sufficient explanations.
Independent t-test was used to compare the lifestyles of veteran and non-veteran men and women in the provinces. Also, Pearson correlation test was used to examine the relationship between the life style and health literacy. All analyses were conducted using SPSS 24.
Findings
Out of 1770 participants, the majority of them were women (58.6%), and the rest were men (41.4%). People had an age range of 15-89 years, and the mean±SD age in each province was as follows: (Gilan=51.09±18.85; Ilam=35.66±13.31; Khorasan Razavi=39.39±16.09; Tehran=44.14±15.39; Isfahan=45.17±19.04). In terms of education, most of these people had diploma degrees (32.1%).
There was no significant difference between the mean scores of the lifestyle in the two groups of veterans and non-veterans in all five provinces studied (p<0.05). Overall, the mean±SD scores of the lifestyle in the male veteran group were higher than the non-veteran group (p<0.05), although the difference between the means was small and was only significant for the large sample size (Table 1).
Also, there was no significant difference between the mean lifestyle scores in the two groups of female veterans and non-veterans in all five provinces studied except Tehran and Ilam (p<0.05). However, the difference between the means was small, and the significance was only due to the large sample size. In general, there was no significant difference between the mean scores of the lifestyle in the two groups of female veterans and female non-veterans (p<0.05) (Table 1).
There was a direct and significant relationship between health literacy of veterans and non-veterans and their lifestyle (p<0.001). The output of this test was significant in Tehran, Khorasan Razavi, and Gilan provinces (Table 2). Also, the results of the relationship between participants' health literacy and their lifestyle in Ilam province indicate that this relationship was significant only in the non-veteran group (p<0.05).
Table 1) Comparison results of the lifestyle and health literacy scores in the two groups of veterans and non-veterans in terms of the province (N=1770)
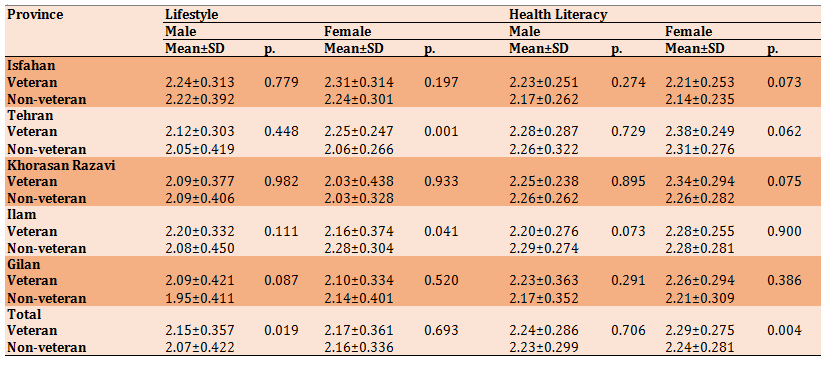
Table 2) Results of Pearson correlation coefficient for the relationship between health literacy and lifestyle of veteran and non-veteran groups
Discussion
The present study was conducted to investigate the correlation between lifestyle and health literacy among veterans and non-veterans and their families and to examine the differences in the lifestyle of their families in 2018.
The findings show that there is a significant correlation between lifestyle and health literacy of veterans and non-veterans. In explaining this finding, it could be stated that behaviors such as avoiding drinking alcohol and smoking, doing a proper diet, and many other positive activities outside the health care system result in a healthy lifestyle [21]. However, these measures are not just a personal choice but are influenced by many structural factors, such as the extent to which people have good health literacy, which leads people to adopt a healthy lifestyle. Because people with good health literacy will have better management of their diet and better nutritional performance. Also, due to their awareness and knowledge, such people automatically observe personal health tips and regularly visit physicians and psychiatrists, helping them have a higher quality of lifestyle both physically and mentally. Good health literacy allows them to spend more time on exercise and physical activity [22], manage the psychological pressures caused by the difficult physical conditions and the many ups and downs around themselves and their families, and have more power to reduce stress and develop psychological adjustment. Our findings are also in line with the results of a study by Von Wagner et al. [23] in the United Kingdom, who believed that there is a relationship between fruit and vegetable consumption and health literacy. Gibers et al. [24] also showed that having health literacy is an influential factor and is coordinated with physical activities. Our findings also confirm Suka et al. [25] in Japan, who found that people with higher health literacy were more physically active.
In addition, our findings indicate that there was no significant difference between the mean scores of lifestyle in the two groups of female veterans and female non-veterans (p<0.05), while the mean scores of lifestyle in the group of male veterans were higher than the group of male non-veterans (p<0.05). However, this difference between the means was small and was significant only due to the large sample size. Nevertheless, due to the sensitivity of the conditions and situation of the veterans, it was expected that the average scores of the lifestyle of the two groups of veterans and non-veterans would be different. It was also expected that the average scores of the veterans' lifestyle were higher than non-veterans for the due attention given to such people during hard and painful enduring years by the state authorities; however, the results were not as expected. Since health behaviors, as a part of the general system of human behaviors and interactions, are influenced by the culture of the society, it seems that the dominant culture of the society regarding healthy behaviors and lifestyles has also influenced the possible differences between the two groups of veterans and non-veterans, eliminating any significant difference. In this regard, Weber believes that lifestyle is a kind of behavior, and life opportunities provide the basis for a healthy behavioral style. These life opportunities include physical conditions, social conditions, and age [26].
According to the existing evidence, it seems that not enough attention has been paid to the life opportunities of the veterans. It is then necessary to give more attention to the lifestyle of the veterans by taking care of the conditions to increase opportunities related to a healthy lifestyle for the veterans.Table 2) Results of Pearson correlation coefficient for the relationship between health literacy and lifestyle of veteran and non-veteran groups
Discussion
The present study was conducted to investigate the correlation between lifestyle and health literacy among veterans and non-veterans and their families and to examine the differences in the lifestyle of their families in 2018.
The findings show that there is a significant correlation between lifestyle and health literacy of veterans and non-veterans. In explaining this finding, it could be stated that behaviors such as avoiding drinking alcohol and smoking, doing a proper diet, and many other positive activities outside the health care system result in a healthy lifestyle [21]. However, these measures are not just a personal choice but are influenced by many structural factors, such as the extent to which people have good health literacy, which leads people to adopt a healthy lifestyle. Because people with good health literacy will have better management of their diet and better nutritional performance. Also, due to their awareness and knowledge, such people automatically observe personal health tips and regularly visit physicians and psychiatrists, helping them have a higher quality of lifestyle both physically and mentally. Good health literacy allows them to spend more time on exercise and physical activity [22], manage the psychological pressures caused by the difficult physical conditions and the many ups and downs around themselves and their families, and have more power to reduce stress and develop psychological adjustment. Our findings are also in line with the results of a study by Von Wagner et al. [23] in the United Kingdom, who believed that there is a relationship between fruit and vegetable consumption and health literacy. Gibers et al. [24] also showed that having health literacy is an influential factor and is coordinated with physical activities. Our findings also confirm Suka et al. [25] in Japan, who found that people with higher health literacy were more physically active.
In addition, our findings indicate that there was no significant difference between the mean scores of lifestyle in the two groups of female veterans and female non-veterans (p<0.05), while the mean scores of lifestyle in the group of male veterans were higher than the group of male non-veterans (p<0.05). However, this difference between the means was small and was significant only due to the large sample size. Nevertheless, due to the sensitivity of the conditions and situation of the veterans, it was expected that the average scores of the lifestyle of the two groups of veterans and non-veterans would be different. It was also expected that the average scores of the veterans' lifestyle were higher than non-veterans for the due attention given to such people during hard and painful enduring years by the state authorities; however, the results were not as expected. Since health behaviors, as a part of the general system of human behaviors and interactions, are influenced by the culture of the society, it seems that the dominant culture of the society regarding healthy behaviors and lifestyles has also influenced the possible differences between the two groups of veterans and non-veterans, eliminating any significant difference. In this regard, Weber believes that lifestyle is a kind of behavior, and life opportunities provide the basis for a healthy behavioral style. These life opportunities include physical conditions, social conditions, and age [26].
Conclusion
There is a correlation between health literacy and the lifestyle in veterans' families and non-veterans families, while there is no difference between the lifestyles in the two groups.
Acknowledgments: We would like to thank all participants in this research.
Ethical Permissions: The University/Regional Research Ethics Committee Veterans and martyr affair foundation (VMFA) [Process No: IR.ISAAR.REC.1398.002].
Conflicts of Interests: The authors declared no potential conflicts of interest for this article's research, authorship, and/or publication.
Authors’ Contributions: Afshani A. (First Author), Introduction Writer/Methodologist/Main Researcher (50%); Shiri H. (Second Author), Introduction Writer/
Statistical Analyst (30%); Hosseini-Motlagh S. (Third Author), Methodologist/Discussion Writer (20%).
Funding/Support: This research was financially supported by the Veterans and Martyrs affair foundation (VMFA), Iran (Grant number: 1397.10.01-430/820/1951).
References
1. Ghasemiyani B, Aghdasi AN. Comparison of resilience, self-differentiation, and health-promoting lifestyle in children of the chemical warfare veterans, non-chemical veterans, prisoners of war and normal population. Iran J War Public Health. 2019;11(4):215-22. [Persian] [Link] [DOI:10.29252/ijwph.11.4.215]
2. Abedini Baltork M, Mir Shamsi FS. Correlation between resilience and mental health with lifestyle and parenting styles of veterans' spouses a case study of Ardakan city. Iran J War Public Health. 2019;11(3):161-7. [Persian] [Link] [DOI:10.29252/ijwph.11.3.161]
3. Hansen E, Easthope G. Lifestyle in medicine. London: Routledge; 2007. [Link] [DOI:10.4324/9780203002841]
4. Abbaszadeh M, Alizadeh Eghdam MB, Badri Gargari R, Vadadahir A. Investigating social and cultural factors affecting the self-care life style of citizens. J Stud Soc Cult Dev. 2012;1(1):119-41. [Persian] [Link]
5. Khaniabad Z, Amiri H, Kakabraee K. Causal model of quality of life in veterans of the nervous system in the aging process of Kermanshah province. Iran J War Public Health. 2020;12(1):35-42. [Persian] [Link] [DOI:10.29252/ijwph.12.1.35]
6. Amoah PA, Phillips DR, Gyasi RM, Koduah AO, Edusei J. Health literacy and self-perceived health status among street youth in Kumasi, Ghana. Cogent Med. 2017;4(1):1275091. [Link] [DOI:10.1080/2331205X.2016.1275091]
7. Mohamadlo A, Batooli Z, Ramezankhani A. The analysis and review of the literatures in the field of health literacy. J Mod Med Inf Sci. 2020;6(2):58-72. [Persian] [Link] [DOI:10.29252/jmis.6.2.58]
8. Ratzan SC, Parker RM. Health literacy-identification and response. J Health Commun. 2006;11(8):713-5. [Link] [DOI:10.1080/10810730601031090] [PMID]
9. Tavousi M, Ebadi M, Azin A, Shakerinejad G, Hashemi A, Fattahi E, et al. Definitions of health literacy: A review of the literature. PAYESH. 2014;13(1):119-24. [Persian] [Link]
10. Klinker CD, Aaby A, Ringgaard LW, Hjort AV, Hawkins M, Maindal HT. Health literacy is associated with health behaviors in students from vocational education and training schools: A Danish population-based survey. Int J Environ Res Public Health. 2020;17(2):671. [Link] [DOI:10.3390/ijerph17020671] [PMID] [PMCID]
11. Kudo N, Yokokawa H, Fukuda H, Hisaoka T, Isonuma H, Naito T. Analysis of associations between health literacy and healthy lifestyle characteristics among Japanese outpatients with lifestyle‐related disorders. J Gen Fam Med. 2016;17(4):299-306. [Link] [DOI:10.14442/jgfm.17.4_299]
12. Wang C, Kane RL, Xu D, Meng Q. Health literacy as a moderator of health-related quality of life responses to chronic disease among Chinese rural women. BMC Womens Health. 2015;15(1):1-8. [Link] [DOI:10.1186/s12905-015-0190-5] [PMID] [PMCID]
13. Shieh C, Halstead JA. Understanding the impact of health literacy on women's health. J Obstet Gynecol Neonatal Nurs. 2009;38(5):601-10. [Link] [DOI:10.1111/j.1552-6909.2009.01059.x] [PMID]
14. Khodabakhshi-Koolaee A, Bahari M, Falsafinejad MR, Shahdadi H. The relationship of quality of life with health literacy in male patients with type II diabetes: A cross-sectional study in Harsin city, 2015. J Diabetes Nurs. 2016;4(4):10-20. [Persian] [Link]
15. Afshani S, Hosseini S. Comparing the lifestyle of veteran and non-veteran families in Tehran. TOLOOE BEHDASHT. 2020;19(4):26-36. [Persian] [Link] [DOI:10.18502/tbj.v19i4.4518]
16. Ministry of interior. The provinces of the country were divided into 5 large regions [Internet]. Tehran: Ministry of Interior; 2014 [cited 2019 Sep 26]. Available from: yun.ir/scsojd. [Persian] [Link]
17. Lali M, Abedi A, Kajbaf MB. Construction and validation of the lifestyle questionnaire (LSQ). Psychol Res. 2012;15(1):64. [Persian] [Link]
18. Hoseinai A, Farnoush F, Zare M, Bahonar A. Study of relationship between life style and communicational technologies abuse, and mental health among Islamic Azad university students of Tehran city. Med Sci J Islam Azad Univ Tehran Med Branch. 2018;28(2):145-52. [Persian] [Link] [DOI:10.29252/iau.28.2.145]
19. Kordestani D. Comparing the resilience, life style and life quality among cardiovascular patients and normal people. YAFTE. 2018;19(5):71-80. [Persian] [Link]
20. Chinn D, McCarthy C. All aspects of health literacy scale (AAHLS): Developing a tool to measure functional, communicative and critical health literacy in primary healthcare settings. Patient Educ Couns. 2013;90(2):247-53. [Link] [DOI:10.1016/j.pec.2012.10.019] [PMID]
21. Cockerham WC. Medical sociology. New York: Routledge; 2017. [Link] [DOI:10.4324/9781315618692]
22. Norozi S, Rezaei R, Safa L. Mediation effect of healthy lifestyle in the relationship between health literacy and rural women's health-related quality of life in west Islam Abad township. J Womens Stud Sociol Psychol. 2017;15(3):1-30. [Persian] [Link]
23. Von Wagner C, Knight K, Steptoe A, Wardle J. Functional health literacy and health-promoting behaviour in a national sample of British adults. J Epidemiol Community Health. 2007;61(12):1086-90. [Link] [DOI:10.1136/jech.2006.053967] [PMID] [PMCID]
24. Geboers B, Reijneveld SA, Jansen CJ, De Winter AF. Health literacy is associated with health behaviors and social factors among older adults: Results from the life lines cohort study. J Health Commun. 2016;21(Suppl 2):45-53. [Link] [DOI:10.1080/10810730.2016.1201174] [PMID]
25. Suka M, Odajima T, Okamoto M, Sumitani M, Igarashi A, Ishikawa H, et al. Relationship between health literacy, health information access, health behavior, and health status in Japanese people. Patient Educ Couns. 2015;98(5):660-8. [Link] [DOI:10.1016/j.pec.2015.02.013] [PMID]
26. Hendry LB. Young people's leisure and lifestyles. New York: Routledge; 1993. [Link]
Send email to the article author