
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

0.5
Cite Score
SJR: 0.129 / SNIP: 0.140
Volume 13, Issue 2 (2021)
Iran J War Public Health 2021, 13(2): 145-153 |
Back to browse issues page
Article Type:
Subject:




History
Received: 2021/05/15 | Accepted: 2021/08/1 | Published: 2021/10/1
Received: 2021/05/15 | Accepted: 2021/08/1 | Published: 2021/10/1
How to cite this article
Satkin M, Ghanei M, Salesi M, Borna H, Ebadi A. Quality of Life in the Iranian Mustard Gas Victims; A Meta-Analysis. Iran J War Public Health 2021; 13 (2) :145-153
URL: http://ijwph.ir/article-1-967-en.html
URL: http://ijwph.ir/article-1-967-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Behavioral Sciences Research Center, Lifestyle Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran
2- Chemical Injuries Research Center, Systems Biology and Poisonings Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran
3- “Behavioral Sciences Research Center, Lifestyle Institute” and “Nursing Faculty”, Baqiyatallah University of Medical Sciences, Tehran, Iran
2- Chemical Injuries Research Center, Systems Biology and Poisonings Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran
3- “Behavioral Sciences Research Center, Lifestyle Institute” and “Nursing Faculty”, Baqiyatallah University of Medical Sciences, Tehran, Iran
Full-Text (HTML) (1239 Views)
Introduction
Sulfur mustard, bis (2-chloroethyl) sulfide (SM), as an alkylating agent, has been the most widely used chemical weapon agent (CWA) between 70 different chemical warfare agents [1, 2]. SM is a strong alkylation agent with high absorbance and impact on lungs, eyes and skin. It may also be absorbed through the gastrointestinal tract following consumption of contaminated food. It is one of the major chemical warfare agents developed and used during World War I (1914-1919) [3, 4]. The first usage of SM was in 1917 by the Natzi army against allied forces in Ypres, Belgium [5]. Also, the Egyptian forces used SM in Yemen during World War II (1939-1945) [6]. Nevertheless, the highest unconventional application of SM occurred in the Iran-Iraq war (1980-1988). According to international statistics, more than 100 thousand injured are suffering from this chemical currently [7].
Respiratory tract injury (42.5%), eyes (39.3%), and skin (24.5%) are the most common late complication of SM inhalation [8, 9]. Respiratory tract injury is the most 70% late complication of SM inhalation that causing disability is pulmonary disorders in which the main underlying pathology is Cough, increased sputum, respiratory volume reduction, bronchiolitis obliterans (BO) and chronic obstructive pulmonary disease (COPD) [5, 10, 11].
Quality-of-life (QOL) has many different contexts for different people. Several factors may involve the QOL [12]. General dimensions of quality of life are physical, mental, social and spiritual. Injuries induced by chemical weapons can alter people's QOL and cause chronic and progressive disorders [13]. QOL in SM patients decreased further with obstructive airway disease and decreases during sleep and frequent awakenings and obstructive sleep apnea (OSA) [14, 15]. OSA is a common respiratory disorder during sleep with breathing or shortness of breath during sleep is characterized by frequent and usually takes 20-40 seconds [16-18].
Except for many physical complications caused by CWA, psychological events are more critical. Psychological consequences will lead to the decrease of l QOL and may even continue for two generations [19].
Improve patient satisfaction and improve the quality of life in patients with increased respiratory problems exposed to the SM [20].
Based on previous studies, the physical injuries, sleep disorders, drug addiction, having no plans for the future, interfering with everyday life, self-esteem, paranoia, anger, and indifference and meaningless in life, lifestyle changes, depression, invasion, nervousness, confusion, and maladaptive life are direct and indirect SM upon QOL in patients [19-22]. Studies have shown that there is no correlation between the occurrence of pathological findings and QOL in sulfur mustards exposer patients. Also has been shown to reduce Respiratory tract injury improves sleep and quality of life of SM and COPD patients [23]. In this meta-analysis paper, we document a series of SM clinical findings and the review impact of SM on the QOL of these patients.
Information and Methods
This meta-analysis was based on the instructions introduced by York University [24], examines the QOL of Iranian chemical gas victims affected by mustard gas in 2019. The texts were available with specific terms and formulas of search searched. To build a formula consulted with two experts specialized in fields of psychology and medical science. The search was done through the Persian and English sources such as IranMedex, Magiran, SID, PubMed, Scopus, and Google Scholar with specific terms and designed search formula until the year 2016. The terms such as "Quality of Life", "Chemical Warfare Agents", "Chemical Warfare", "Chemical veterans", "Chemical weapon", "Chemical injuries", "Mustard" and "Mustard Gas" were searched in Scientific Information Database (SID), IranMedex and Magiran. Also, the manual search had been done through journals like "Iranian Journal of War and Public Health", "Journal of military medicine," and "Journal of Behavioral Sciences". Then the advanced search continued on Google Scholar, Scopus, and PubMed with specific terms. The eligible studies consist of all precise studies related to the QOL of chemical gas victims. Hence other documents such as books, article reviews, and reports were removed as they were not suitable to answer the research question, time limits, and lack of possibility of qualitative assessment. To preserve the neutrality of the research and reduce the possible errors in data gathering in the research, the topics and abstracts were assessed by two researchers, and the studies that did not have the research criteria were removed.
The data was extracted based on the standard form designed previously for gathering them. This form was designed by the research group, including items such as writer's name, the topic of the study, year of publish, name of the journal, criteria of input and output number of sample, and type of questionnaires. The remained studies had been retrieved and were scrutinized to be eligible by the research group. Full texts were not masked to the author or publication. The Discrepancies were solved by the third researcher. The articles were assessed according to the evaluating checklist by the National Institutes of Health (NIH) [25]. This checklist includes 14 criteria to evaluate the articles based on qualitative standards; the checklist had been designed based on a selective strategy of York University by our planning and executive team. In the assessment phase, the articles within a minimum of 60% of the total score were chosen for the analysis. The questionnaires that used in the research are Medical Outcome Study Short Form-36 (SF-36) and St. George's Respiratory Questionnaire (SGRQ) [26-31].
After the systematic review of the texts, based on the question of the research and the criteria designed in the qualitative checklist, 21 articles were chosen. Fourteen of them were removed from the studies (five were removed due to unreasonable methods and lack of enough information, nine were removed as they did not have the minimum score from the checklist); at the end, seven articles [34-40] remained with the qualitative assessment provided before and chosen for the analysis (Figure 1). In the results, the articles [34-40] were named A1 to A7, respectively. We contacted the writers of the three articles [35, 36, 39] for more information because of justification and further explanation for their outputs and inputs and how the articles were studied. Also, some Persian articles in this field did not have the necessary writing qualifications and were reported unclear.
Simotinously the results were imported on EndNote X7 software. The number of studies was too small to assess publication bias reliably; all analyses were conducted using STATA 12.1.
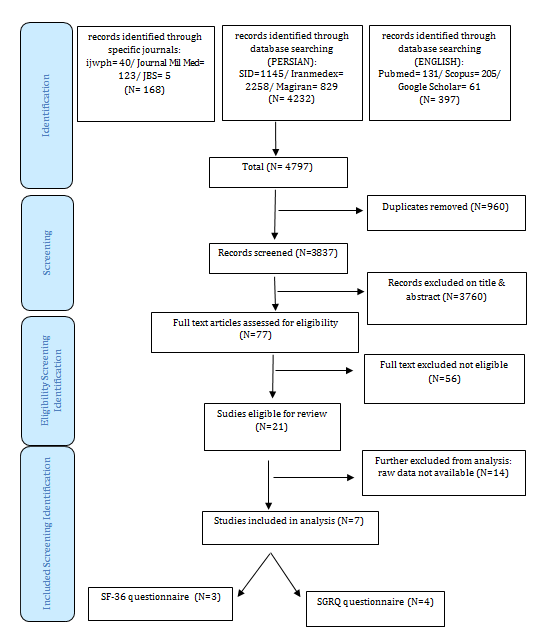
Figure 1) Study selection Diagram
Sulfur mustard, bis (2-chloroethyl) sulfide (SM), as an alkylating agent, has been the most widely used chemical weapon agent (CWA) between 70 different chemical warfare agents [1, 2]. SM is a strong alkylation agent with high absorbance and impact on lungs, eyes and skin. It may also be absorbed through the gastrointestinal tract following consumption of contaminated food. It is one of the major chemical warfare agents developed and used during World War I (1914-1919) [3, 4]. The first usage of SM was in 1917 by the Natzi army against allied forces in Ypres, Belgium [5]. Also, the Egyptian forces used SM in Yemen during World War II (1939-1945) [6]. Nevertheless, the highest unconventional application of SM occurred in the Iran-Iraq war (1980-1988). According to international statistics, more than 100 thousand injured are suffering from this chemical currently [7].
Respiratory tract injury (42.5%), eyes (39.3%), and skin (24.5%) are the most common late complication of SM inhalation [8, 9]. Respiratory tract injury is the most 70% late complication of SM inhalation that causing disability is pulmonary disorders in which the main underlying pathology is Cough, increased sputum, respiratory volume reduction, bronchiolitis obliterans (BO) and chronic obstructive pulmonary disease (COPD) [5, 10, 11].
Quality-of-life (QOL) has many different contexts for different people. Several factors may involve the QOL [12]. General dimensions of quality of life are physical, mental, social and spiritual. Injuries induced by chemical weapons can alter people's QOL and cause chronic and progressive disorders [13]. QOL in SM patients decreased further with obstructive airway disease and decreases during sleep and frequent awakenings and obstructive sleep apnea (OSA) [14, 15]. OSA is a common respiratory disorder during sleep with breathing or shortness of breath during sleep is characterized by frequent and usually takes 20-40 seconds [16-18].
Except for many physical complications caused by CWA, psychological events are more critical. Psychological consequences will lead to the decrease of l QOL and may even continue for two generations [19].
Improve patient satisfaction and improve the quality of life in patients with increased respiratory problems exposed to the SM [20].
Based on previous studies, the physical injuries, sleep disorders, drug addiction, having no plans for the future, interfering with everyday life, self-esteem, paranoia, anger, and indifference and meaningless in life, lifestyle changes, depression, invasion, nervousness, confusion, and maladaptive life are direct and indirect SM upon QOL in patients [19-22]. Studies have shown that there is no correlation between the occurrence of pathological findings and QOL in sulfur mustards exposer patients. Also has been shown to reduce Respiratory tract injury improves sleep and quality of life of SM and COPD patients [23]. In this meta-analysis paper, we document a series of SM clinical findings and the review impact of SM on the QOL of these patients.
Information and Methods
This meta-analysis was based on the instructions introduced by York University [24], examines the QOL of Iranian chemical gas victims affected by mustard gas in 2019. The texts were available with specific terms and formulas of search searched. To build a formula consulted with two experts specialized in fields of psychology and medical science. The search was done through the Persian and English sources such as IranMedex, Magiran, SID, PubMed, Scopus, and Google Scholar with specific terms and designed search formula until the year 2016. The terms such as "Quality of Life", "Chemical Warfare Agents", "Chemical Warfare", "Chemical veterans", "Chemical weapon", "Chemical injuries", "Mustard" and "Mustard Gas" were searched in Scientific Information Database (SID), IranMedex and Magiran. Also, the manual search had been done through journals like "Iranian Journal of War and Public Health", "Journal of military medicine," and "Journal of Behavioral Sciences". Then the advanced search continued on Google Scholar, Scopus, and PubMed with specific terms. The eligible studies consist of all precise studies related to the QOL of chemical gas victims. Hence other documents such as books, article reviews, and reports were removed as they were not suitable to answer the research question, time limits, and lack of possibility of qualitative assessment. To preserve the neutrality of the research and reduce the possible errors in data gathering in the research, the topics and abstracts were assessed by two researchers, and the studies that did not have the research criteria were removed.
The data was extracted based on the standard form designed previously for gathering them. This form was designed by the research group, including items such as writer's name, the topic of the study, year of publish, name of the journal, criteria of input and output number of sample, and type of questionnaires. The remained studies had been retrieved and were scrutinized to be eligible by the research group. Full texts were not masked to the author or publication. The Discrepancies were solved by the third researcher. The articles were assessed according to the evaluating checklist by the National Institutes of Health (NIH) [25]. This checklist includes 14 criteria to evaluate the articles based on qualitative standards; the checklist had been designed based on a selective strategy of York University by our planning and executive team. In the assessment phase, the articles within a minimum of 60% of the total score were chosen for the analysis. The questionnaires that used in the research are Medical Outcome Study Short Form-36 (SF-36) and St. George's Respiratory Questionnaire (SGRQ) [26-31].
After the systematic review of the texts, based on the question of the research and the criteria designed in the qualitative checklist, 21 articles were chosen. Fourteen of them were removed from the studies (five were removed due to unreasonable methods and lack of enough information, nine were removed as they did not have the minimum score from the checklist); at the end, seven articles [34-40] remained with the qualitative assessment provided before and chosen for the analysis (Figure 1). In the results, the articles [34-40] were named A1 to A7, respectively. We contacted the writers of the three articles [35, 36, 39] for more information because of justification and further explanation for their outputs and inputs and how the articles were studied. Also, some Persian articles in this field did not have the necessary writing qualifications and were reported unclear.
Simotinously the results were imported on EndNote X7 software. The number of studies was too small to assess publication bias reliably; all analyses were conducted using STATA 12.1.
Figure 1) Study selection Diagram
Findings
In 7 studies that were applied on Iranian male victims (n=1241), their age average had been recorded as 45.66 (rang: 41.18-48.08), which they age between 44.12±4.9 to 48.08±7.8. Also, the tool to measure the QOL between 681 victims for three of the studies had been the SF-36 questionnaire, and in the other four studies, the SGRQ questionnaire had been used for 560 victims of chemical weapons (mustard gas).
The results of the mustard gas victims (MGV) in Iran based on the SF-36 questionnaire showed that the pooled score of all sub-scales was lower than the average (lower than 50). The pooled score of pcs in MGV in Iran was 28.33 (95% CI: 24.02-32.63), whereas the MCS between these victims was 35.83 (95% CI: 29.07-42.59). The chemical gas victims had a lower score in pcs comparing to MCS.
The chemical gas victims in the physical component recorded a low score in the role function-physical subscale, and the general health subscale was 21.76 (95% CI: 19.99-23.53 and 25.44 (95% CI: 19.77-31.11), respectively. This showed that the chemical gas victims enjoy an appropriate situation regarding the subscales. All of the studies showed that the General Health and Role function-physical in the physical component had the lowest scores. The victims had the highest score in the physical component in the physical functioning subscale, which was 40.13 (95% CI: 31.53-48.73). Also, the chemical victims in the mental component dimension in the role function-emotional and vitality subscales were 31.36 (95% CI: 17.70-45.01) and 34.59 (95% CI: 28.58-40.60) sequentially, which were respectively low scores. This proves that the chemical victims had an unsuitable situation in the subscales. All studies showed that the mental component's role function-emotional and vitality subscales had the least scores. Also, these victims had the highest scores regarding the social functioning subscale 44.83 (95% CI: 43.04-46.63) in mental functioning.
In the SF-36 questionnaire, the lower scores showed the inappropriate situation of life; the results prove that the role function-physical subscale in the physical component and the role function-emotional in the mental component had the most unfavorable status. The combined results of QOL based on SF-36 were reported in Table 1.
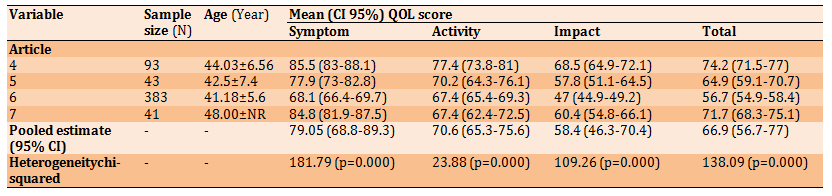
The results of the SGRQ QOL questionnaire show that the pooled score of QOL of the chemical gas victims by mustard gas in Iran was 66.9 (95% CI: 56.7-77). The pooled estimated score of the chemical gas victims in the symptom sub-scale was 79.05 (95% CI: 68.8-89.3), which was higher than the activity sub-scale with an average score of 70.6 (95% CI: 65.3-75.6) and the average of the impact sub-scale 58.3 (95% CI: 46.3-70.4). The higher score in this questionnaire was an indication of an unfavorable situation; the chemical gas victims in the symptom sub-scale had more difficulties
(Table 2)
In 7 studies that were applied on Iranian male victims (n=1241), their age average had been recorded as 45.66 (rang: 41.18-48.08), which they age between 44.12±4.9 to 48.08±7.8. Also, the tool to measure the QOL between 681 victims for three of the studies had been the SF-36 questionnaire, and in the other four studies, the SGRQ questionnaire had been used for 560 victims of chemical weapons (mustard gas).
The results of the mustard gas victims (MGV) in Iran based on the SF-36 questionnaire showed that the pooled score of all sub-scales was lower than the average (lower than 50). The pooled score of pcs in MGV in Iran was 28.33 (95% CI: 24.02-32.63), whereas the MCS between these victims was 35.83 (95% CI: 29.07-42.59). The chemical gas victims had a lower score in pcs comparing to MCS.
The chemical gas victims in the physical component recorded a low score in the role function-physical subscale, and the general health subscale was 21.76 (95% CI: 19.99-23.53 and 25.44 (95% CI: 19.77-31.11), respectively. This showed that the chemical gas victims enjoy an appropriate situation regarding the subscales. All of the studies showed that the General Health and Role function-physical in the physical component had the lowest scores. The victims had the highest score in the physical component in the physical functioning subscale, which was 40.13 (95% CI: 31.53-48.73). Also, the chemical victims in the mental component dimension in the role function-emotional and vitality subscales were 31.36 (95% CI: 17.70-45.01) and 34.59 (95% CI: 28.58-40.60) sequentially, which were respectively low scores. This proves that the chemical victims had an unsuitable situation in the subscales. All studies showed that the mental component's role function-emotional and vitality subscales had the least scores. Also, these victims had the highest scores regarding the social functioning subscale 44.83 (95% CI: 43.04-46.63) in mental functioning.
In the SF-36 questionnaire, the lower scores showed the inappropriate situation of life; the results prove that the role function-physical subscale in the physical component and the role function-emotional in the mental component had the most unfavorable status. The combined results of QOL based on SF-36 were reported in Table 1.
The results of the SGRQ QOL questionnaire show that the pooled score of QOL of the chemical gas victims by mustard gas in Iran was 66.9 (95% CI: 56.7-77). The pooled estimated score of the chemical gas victims in the symptom sub-scale was 79.05 (95% CI: 68.8-89.3), which was higher than the activity sub-scale with an average score of 70.6 (95% CI: 65.3-75.6) and the average of the impact sub-scale 58.3 (95% CI: 46.3-70.4). The higher score in this questionnaire was an indication of an unfavorable situation; the chemical gas victims in the symptom sub-scale had more difficulties
(Table 2)
Table 1) The combined results of SF-36 QOL questionnaire scores (higher scores indicates a better condition)
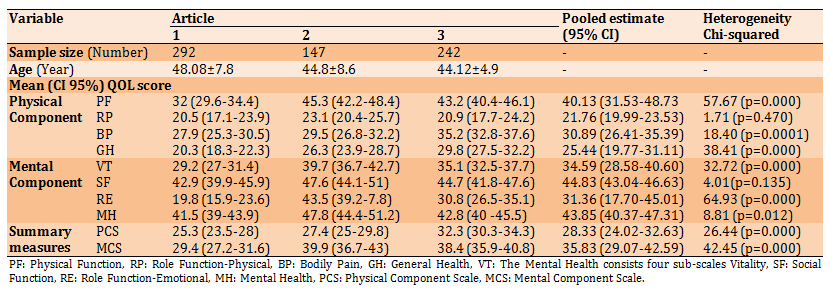
Table 2) the combined results of the SGRQ questionnaire scores (lower scores indicates a better condition)
Discussion
The current study is the first meta-analysis about the chemical gas victims of mustard gas in Iran. This meta-analysis aims to assess the QOL of MGV in Iran. Considering the meta-analysis results in both questionnaires (Generic and Specific), the chemical gas victims by mustard gas have lower QOL in physical components than mental components.
Statistical heterogeneity (p<0.1) was detected in none of the three SGRQ domains; hence, we used the random effect method to combine the scores. According to the meta-analysis results in both SF-36 general QOL questionnaire and the SGRQ dedicated QOL questionnaire, the chemical gas victims by mustard gas had a more unfavorable situation in the physical component than the mental component. In the SF-36 questionnaire, the role function-physical 21.38 (19.8-22.9) and the general health sub-scales and in the SGRQ questionnaire symptom 79.05 (68.8-89.3) and activity 70.6 (65.3-75.6) sub-scales were related to the physical component of QOL that had the most inappropriate status. This proves that the victims had more problems in the physical component compared to the mental component. In table 3, the meta-analysis results were available in addition to the QOL of two groups: the general Iranian male population and COPD patients. For better analysis, the results of the current meta-analysis in the SGRQ QOL questionnaire were compared with the COPD and asthmatic patients in Table 4.
The results show that the average combined scores
Table 3) Comparison between the SF-36 scores between MGV (chemical warfare patients) and a general Iranian population and a COPD Patients population (higher scores indicate a better condition)
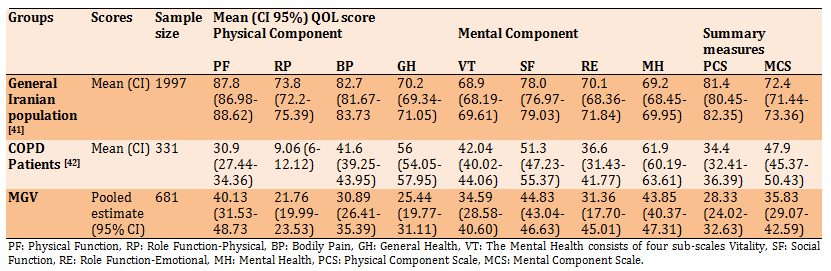
Table 4) Comparison between the SGRQ scores between MGV (chemical warfare patients) and COPD Patients population and asthmatic patients (lower scores indicate a better condition)

in all sub-scales in the SF-36 questionnaire are lower than 50. This means the QOL of chemical gas victims by mustard gas in all sub-scales is low. The chemical gas victims have lower scores in the PCS comparing to the MCS. That means the physical status of the MGV is more inappropriate in comparison to their mental status. There have been few reviews about the chemical gas victims by mustard gas [45]. As a consequence of the chemical gas lesions and chronic respiratory diseases, the disorder in the QOL, especially in the physical component, is expected [34]. Many pieces of research have mentioned factors such as an increase of one-step spirometry parameters, a decrease of FEV1, Bronchiolitis and lack of sports activities that decrease the QOL of chemical gas victims by mustard gas [46]. Other studies also have recorded low physical component sub-scales among the pulmonary patients [47].
The chemical gas victims have the most unsuitable situation in the General Health and Role Function-Physical sub-scales. The Role Function-Physical assesses the limits in doing daily the activities or types of activities [27]. Due to the respiratory complications by the mustard gas, the chemical gas victims cannot do their daily activities easily, which limits and hardens their physical functions. The general Health sub-scale assesses the health of patients, including the current health, the person's point of view about health, and resistance against diseases [27]. Due to the injuries in several body members such as lungs, eyes, skin and nerves, the chemical gas victims of mustard gas are suffering from diseases and body complications. The studies refer the lowest QOL to the victims suffering from different diseases simultaneously [46].
This long chronic status negatively affects the point of view of the patient about his health and decreases the body's resistance against the diseases. The decline of body resistance could cause cancer disease for the chemical gas victims by mustard gas [48, 49].
Also, the chemical gas victims experience an inappropriate situation in the Mental Component, especially in the role Function-Emotional and vitality sub-scales. The Role Function-Emotional sub-scale measures the disorders caused by emotional problems in daily activities such as reducing time for doing activities and performance of activities with lesser accuracy contrary to past habits [27]. The body diseases and complications caused by mustard gas create problems for the chemical gas victims. These emotional problems decrease the patience, accuracy, and quality of the victims' performance [46, 50, 51].
On the other hand, the psychological diseases in MGV such as Post-traumatic stress disorder (PTSD), anxiety and depression are higher than average, which reduce the role Function-Emotional among these victims [50]. Vitality is a concept that measures liveliness and happiness, which are the opposite point of fatigue and exhaustion [27]. For being delighted, a person needs a healthy body and well mind. Usually, the people who have a more healthy body and mind would experience more vitality and happiness. The chemical gas victims by mustard gas feel tired and exhausted due to the late complications and prolonged physical and mental complications [36]. Also, the researches show that the chemical gas victims with a higher percentage of injuries experience a lower QOL [37].
Comparing the average of QOL among the male population in Iran [35] with the combined SF-36 questionnaire sub-scales scores average of QOL in MGV shows that the scores of the chemical gas victims by mustard gas are measured very low in all sub-scales (Table 3). Jafari's studies also prove that the QOL of chemical gas victims by mustard gas is very low in all sub-scales compared to Iran's population [34]. The scoring average of the general public in Iran in the PCS is 81.4 (21.8) and in the MCS is 72.4 (21.9), wheres as in the current study is 28.33 (24.02-32.63) and 35.83 (29.07-42.59), respectively, which shows the significant difference in the scores. Unlike the chemical gas victims, the score of the general public of Iran in the PCS (81.4 (21.8)) is higher than the MCS (72.4 (21.9)). The physical problems among the chemical gas victims by mustard gas are more prominent than mental health problems. This shows that physical status affects the QOL highly. The general population has better QOL due to lack of affection for special physical and mental diseases, but we have compared both groups (chemical gas victims & general population) in the table to show the significant difference between the two.
Also, the comparison between the average of the scores of QOL among COPD patients and combined scores average of SF-36 questionnaire sub-scales in the chemical gas victims by mustard gas (except the Physical functioning and Role Function-Physical subscales) shows that all of the MGV have lower scores compared to the COPD patients [42]. The PCS (34.4 (18.5) and MCS (47.9 (23.5) in the COPD patients are higher than the PCS (28.33 (24.02-32.63)) and MCS (35.83 (29.07-42.59)) among the chemical gas victims by mustard gas which shows the inappropriate situation of MGV (Table 3). The scores of PCS and MCS in both groups are lower than the average, but the scores regarding the chemical gas victims by mustard gas are lower, which shows lower QOL than the COPD patients. These victims have very low scores in the Physical Component, especially in the Physical functioning and role Function-Emotional sub-scales like COPD Patients, whereas in the Bodily Pain and General Health sub-scales, the COPD patients have higher scores. Though COPD patients have more physical problems, their pain tolerance and general health are relatively high. Pain has a minor effect on the daily activities of COPD patients, and they have a better perspective about self-health and higher resistance against diseases [52]. The COPD patients and chemical gas victims have the lowest scores in the Mental Component, especially in Vitality and Role Function-Emotional sub-scales, but the Mental Health status is lower in the chemical gas victims than the COPD patients. Though the Vitality and Role Function-Emotional sub-scales are low in the COPD patients and chemical gas victims, the COPD patients experience more vitality and lesser exhaustion. The chemical gas victims by mustard gas have psychological disorders and war psycho-social complications like PTSD, anxiety, depression [50], and sometimes they experience a combination of disorders that would lead to the decline of their MH, which is not necessarily seen in COPD patients [38, 39].
The results of the SGRQ questionnaire show that the average QOL between the chemicals gas victims by the mustard gas in Iran is 66.9 (95% CI: 56.7-77). This score represents the unfavorable QOL between the chemical gas victims. Other studies also agree with the statement above, and there is consensus between almost all the studies that the score of QOL among the chemical gas victims is low [37-40]. Nevertheless, the difference between these researches is their low scores of QOL. The low QOL could result from pulmonary complications, restriction of movement, shortness of breath, mental disorders and social disorders caused by respiratory diseases and their effect on social performance [45, 46].
Also, the chemical gas victims have the highest score and the most inappropriate situation in the Symptom sub-scale with an average of 79.05 (95% CI: 68.8-89.3). This component is concerned with the effect of respiratory symptoms, their frequency and severity [53]. The most unsuitable situation for the chemical gas victims is in this sub-scale, a complication by mustard gas mainly related to pulmonary and respiratory complications. The studies show that as the severity of the chemical injury increases, the pulmonary complication also increases and as a consequence, the QOL of the chemical gas victims decreases [19, 36-38, 40].
To precisely analyze the results of the meta-analysis in the SGRQ questionnaire were compared with the QOL among the COPD and asthmatic patients with almost the same situation as the MGV (Table 4). Also, to compare the data with one another, the standard deviation (SD) of the COPD and asthmatic patients were changed to the confidence interval (CI) formula. The comparison between the average score of QOL of COPD and asthmatic patients and the QOL of MGV by the SGRQ questionnaire reveals all scores of MGV are higher, which proves their improper situation (Table 4). Though the QOL has been affected strongly by the physical problems both in the COPD and asthmatic patients and the MGV, other special or unique factors have a greater effect on the decline of QOL between the MGV. The studies point to the simultaneous affection to different diseases (like Respiratory, ocular, dermatological and psychological diseases) [36, 37, 39, 52, 54], Skin lesions (like skin blister, irritation, Excoriation and Lichenification) [55], psychological disorders (like PTSD, depression and anxiety) [34, 37-39, 52], disorders in the personal relations (like sexual relation) [55, 56], interpersonal relation and social function disorder [40, 41, 55].
As COPD patients and MGV suffer from respiratory and pulmonary complaints, we suggest more comparative studies on QOL among the two groups. There shall be studies aiming to differentiate the COPD patients and MGV with the help of the SRGQ and SF-36 questionnaires, as both are prevalent questionnaires. Also, designing and implementing interventional studies can be useful in order to scrutiny the interventions on the QOL of MGV. As there is a lack of meta-analysis studies about the chemical gas victims by mustard gas in Iran, we believe this study can be considered the basis for interventional studies. Lack of information about simultaneous and multiple diseases of the chemical gas victims was one of our limitations.
Conclusion
The QOL between the victims of chemical gas by mustard gas in Iran has been very low. These victims have an unsuitable situation both in physical component and a mental component. While they have a better situation in the mental component comparing to the physical component.
Acknowledgments: Hereby, the review team would like to thank all researchers whose studies in the field of chemically injured veterans fostered the current Meta-Analysis. In addition, the authors express sincere gratitude towards all the exposed veterans and their families.
Ethical Permissions: This study had no Ethical Permissions.
Conflict of Interests: The authors declare no conflict of interests.
Authors’ Contributions: Satkin M. (First Author), Main Researcher/Statistical analyst/Discussion Writer (50%); Ghanei M. (Second Author), Assistant Researcher/Discussion Writer (20%); Salesi M. (Third Author), Methodologist/ Statistical analyst (15%); Borna H. (Fourth Author), Introduction Writer/ Assistant Researcher (10%); Ebadi A. (Fifth Author), Methodologist (5%).
Funding/Support: This study had no funding.
Keywords:
Quality of Life [MeSH], Mustard Gas [MeSH], Iran [MeSH], Meta-Analysis [MeSH], Chemical Warfare Agents [MeSH]
References
1. Malhotra RC, Ganesan K, Sugendran K, Swamy RV. Chemistry and toxicology of sulphur mustard: A review. Def Sci J. 2013;49(2):97-116. [Link] [DOI:10.14429/dsj.49.3793]
2. Shadboorestan A. Commentary on: A review on delayed toxic effects of sulfur mustard in Iranian veterans. DARU. 2012;20(1):99. [Persian] [Link] [DOI:10.1186/2008-2231-20-99] [PMID] [PMCID]
3. Stockholm international peace research institute. The problem of chemical and biological warfare: A study of the historical, technical, military, legal and political aspects of CBW, and possible disarmament measures. Boston: Humanities Press; 1973. [Link]
4. Alexander SF. Medical report on the Bari Harbor mustard casualties. Mil Surg. 1947;101(1):1-17. [Link]
5. Aghanouri R, Ghanei M, Aslani J, Keivani-Amine H, Rastegar F, Karkhane A. Fibrogenic cytokine levels in bronchoalveolar lavage aspirates 15 years after exposure to sulfur mustard. Am J Physiol Lung Cell Mol Physiol. 2004;287(6):1160-4. [Link] [DOI:10.1152/ajplung.00169.2003] [PMID]
6. Holmes R, Uitm M, Alam S.The THES ranking: Are they really world class. Asian J Univ Educ. 2006;2(1):1-14. [Link]
7. Khateri S, Ghanei M, Keshavarz S, Soroush M, Haines D. Incidence of lung, eye, and skin lesions as late complications in 34,000 Iranians with wartime exposure to mustard agent. J Occup Environ Med. 2003;45(11):1136-43. [Link] [DOI:10.1097/01.jom.0000094993.20914.d1] [PMID]
8. Ghanei M, Harandi AA. Molecular and cellular mechanism of lung injuries due to exposure to sulfur mustard: A review. Inhal Toxicol. 2011;23(7):363-71. [Link] [DOI:10.3109/08958378.2011.576278] [PMID]
9. Ghanei M, Poursaleh Z, Harandi AA, Emadi SE, Emadi SN. Acute and chronic effects of sulfur mustard on the skin: A comprehensive review. Cutan Ocul Toxicol. 2010;29(4):269-77. [Link] [DOI:10.3109/15569527.2010.511367] [PMID]
10. Ghanei M, Harandi AA. Long term consequences from exposure to sulfur mustard: A review. Inhal Toxicol. 2007;19(5):451-6. [Link] [DOI:10.1080/08958370601174990] [PMID]
11. Bijani K, Moghadamnia AA. Long-term effects of chemical weapons on respiratory tract in Iraq-Iran war victims living in Babol (north of Iran). Ecotoxicol Environ Saf. 2002;53(3):422-4. [Link] [DOI:10.1016/S0147-6513(02)00034-9]
12. Felce D, Perry J. Quality of life: Its definition and measurement. Res Devel Disabil. 1995;16(1):51-74. [Link] [DOI:10.1016/0891-4222(94)00028-8]
13. Rittmeyer A. Quality of life in patients with NSCLC receiving maintenance therapy. Cancers. 2015;7(2):950-62. [Link] [DOI:10.3390/cancers7020817] [PMID] [PMCID]
14. Fleetham J, West P, Mezon B, Conway W, Roth T, Kryger M. Sleep, arousals, and oxygen desaturation in chronic obstructive pulmonary disease. The effect of oxygen therapy. Am Rev Respir Dis. 1982;126(3):429-33. [Link]
15. Kinsman RA, Yaroush RA, Fernandez E, Dirks JF, Schocket M, Fukuhara J. Symptoms and experiences in chronic bronchitis and emphysema. Chest. 1983;83(5):755-61. [Link] [DOI:10.1378/chest.83.5.755] [PMID]
16. Li Q, Wang Q. Sleep related breathing disorders in international classification of sleep disorders-3. Zhonghua Jie He He Hu Xi Za Zhi. 2014;37(12):883-4. [Chinese] [Link]
17. Morrison I, Buskova J, Nevsimalova S, Douglas NJ, Riha RL. Diagnosing narcolepsy with cataplexy on history alone: Challenging the international classification of sleep disorders (ICSD-2) criteria. Eur J Neurol. 2011;18(7):1017-20. [Link] [DOI:10.1111/j.1468-1331.2010.03223.x] [PMID]
18. Shiina K, Tomiyama H, Takata Y, Yoshida M, Kato K, Nishihata Y, et al. Overlap syndrome: Additive effects of COPD on the cardiovascular damages in patients with OSA. Respir Med. 2012;106(9):1335-41. [Link] [DOI:10.1016/j.rmed.2012.05.006] [PMID]
19. Berahmani G, Abed Saeidi ZH, Kheiri AA. Quality of life in chemical warfare victims in Sardasht, Iran. Med J Tabriz Univ Med Sci. 2004;38(62):9-13. [Persian] [Link]
20. Panahi Y, Sahebkar A, Amiri M, Davoudi SM, Beiraghdar F, Hoseininejad SL, et al. Improvement of sulphur mustard-induced chronic pruritus, quality of life and antioxidant status by curcumin: Results of a randomised, double-blind, placebo-controlled trial. Br J Nutr. 2012;108(7):1272-9. [Link] [DOI:10.1017/S0007114511006544] [PMID]
21. Mansour Razavi S, Salamati P, Saghafinia M, Abdollahi M. A review on delayed toxic effects of sulfur mustard in Iranian veterans. DARU. 2012;20(1):51. [Persian] [Link] [DOI:10.1186/2008-2231-20-51] [PMID] [PMCID]
22. Madarshahian F. Comparison of coping with direct and indirect consequences of war stress in later life between chemical and physical war injureds. J Mil Med. 2003;5(2):117-20. [Persian] [Link]
23. Charokopos N, Leotsinidis M, Pouli A, Tsiamita M, Karkoulias K, Spiropoulos K. Periodic limb movement during sleep and chronic obstructive pulmonary disease. Sleep Breath. 2008;12(2):155-9. [Link] [DOI:10.1007/s11325-007-0151-9] [PMID]
24. Centre for reviews and dissemination. Systematic reviews: CRD's guidance for undertaking reviews in health care. York: Centre for Reviews & Dissemination; 2009. [Link]
25. National heart lung and blood institute. Quality assessment tool for observational cohort and cross-sectional studies [Internet]. Bethesda: National Heart Lung and Blood Institute; 2014 [cited: Unknown]. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. [Link]
26. McHorney CA, Ware Jr JE, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II psychometric and clinical tests of validity in measuring physical and mental health constructs. Med Care. 1993;31(3):247-63. [Link] [DOI:10.1097/00005650-199303000-00006] [PMID]
27. Ware Jr JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I conceptual framework and item selection. Med Care. 1992;30(6):473-83. [Link] [DOI:10.1097/00005650-199206000-00002]
28. Ware JE, Kosinski M, Gandek B, Aaronson NK, Apolone G, Bech P, et al. The factor structure of the SF-36 Health Survey in 10 countries: Results from the IQOLA project. J Clin Epidemiol. 1998;51(11):1159-65. [Link] [DOI:10.1016/S0895-4356(98)00107-3]
29. Ferrer M, Alonso J, Prieto L, Plaza V, Monso E, Marrades R, et al. Validity and reliability of the St George's respiratory questionnaire after adaptation to a different language and culture: The Spanish example. Eur Respir J. 1996;9(6):1160-6. [Link] [DOI:10.1183/09031936.96.09061160] [PMID]
30. Ferrer M, Villasante C, Alonso J, Sobradillo V, Gabriel R, Vilagut G, et al. Interpretation of quality of life scores from the St George's respiratory questionnaire. Eur Respir J. 2002;19(3):405-13. [Link] [DOI:10.1183/09031936.02.00213202] [PMID]
31. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation. Am Rev Respir Dis. 1992;145(6):1321-7. [Link] [DOI:10.1164/ajrccm/145.6.1321] [PMID]
32. Clark TS, Linzer DA. Should I use fixed or random effects. Politc Sci Res Methods. 2015;3(2):399-408. [Link] [DOI:10.1017/psrm.2014.32]
33. Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Stat Med. 2002;21(11):1539-58. [Link] [DOI:10.1002/sim.1186] [PMID]
34. Jafari F, Guitynavard F, Soroush M, Muosavi B. Quality of life in chemical war victims with sever pulmonary damage. TEBE JANBAZ. 2012;4(13):46-52. [Persian] [Link]
35. Mousavi B, Soroush MR, Montazeri A. Quality of life in chemical warfare survivors with ophthalmologic injuries: The first results form Iran chemical warfare victims health assessment study. Health Qual Life Outcomes. 2009;7:2. [Link] [DOI:10.1186/1477-7525-7-2] [PMID] [PMCID]
36. Ebadi A, Moradian T, Mollahadi M, Saeed Y, Refahi AA. Quality of life in Iranian chemical warfare veteran's. Iran Red Crescent Med J. 2014;16(5):5323. [Link] [DOI:10.5812/ircmj.5323]
37. Mehdizadeh S, Salaree M, Ebadi A, Aslan J, Jafari N. Health-related quality of life in chemical warfare victims with bronchiolitis obliterans. Iran J Nurs Res. 2011;6(21):6-14. [Persian] [Link]
38. Ataran D, Khajedaloui M, Mazloomi M, Jafarzadeh R. Health-related quality of life in patients with chemical warfare-induced chronic obstructive pulmonary disease. Arch Iran Med. 2006;9(4):359-63. [Persian] [Link]
39. Tavallaie SA, Assari S, Habibi M, Alaeddini F. Health related quality of life in subjects with chronic bronchiolitis obliterans due to chemical warfare agents. J Mil Med. 2006;7(4):313-20. [Persian] [Link]
40. Arefnasab Z, Ghanei M, Noorbala AA, Alipour A, Babamahmoodi A. Correlation of spirometry and health- related quality of life with mental health in respiratory chemical damaged veterans. J Mazandaran Univ Med Sci. 2013;23(107):48-55. [Persian] [Link]
41. Mousavi B, Khateri S, Soroush M, Amini R, Masumi M, Montazeri A. Comparing quality of life between survivors of chemical warfare exposure and conventional weapons: Results of a national study from Iran. J Med Chem Biol Radiol Def. 2011;8:1-7. [Link]
42. Masroor Roudsari D, Rafii F, Fadaeeaghdam N, Hoseini AF. Health-related quality of life in patients with chronic obstructive pulmonary disease. Iran J Nurs. 2012;25(76):19-27. [Persian] [Link]
43. Fallah Tafti S, Cheraghvandi A, Mokri B, Talischi F. Determining the validity and specificity of the Persian version of Saint George's respiratory questionnaire. J Asthma. 2011;48(6):589-92. [Link] [DOI:10.3109/02770903.2011.587578] [PMID]
44. Mirdamadi M, Rahimi B, Safavi E, Abtahi H, Peiman S. Correlation of cardiopulmonary exercise testing parameters with quality of life in stable COPD patients. J Thorac Dis. 2016;8(8):2138-45. [Link] [DOI:10.21037/jtd.2016.07.07] [PMID] [PMCID]
45. Razavi SM, Negahban Z, Pirhosseinloo M, Razavi MS, Hadjati G, Salamati P. Sulfur mustard effects on mental health and quality of life: A review. Iran J Psychiatry Behav Sci. 2014;8(3):11-21. [Link]
46. Satkin M, Ghanei M, Ebadi A, Allahverdi S, Elikaei M. The quality of life of mustard gas victims: A systematic review. TANAFFOS. 2017;16(2):115-26. [Persian] [Link]
47. Stahl E, Lindberg A, Jansson SA, Ronmark E, Svensson K, Andersson F, et al. Health-related quality of life is related to COPD disease severity. Health Qual Life Outcomes. 2005;3:56. [Link] [DOI:10.1186/1477-7525-3-56] [PMID] [PMCID]
48. Adair FE, Bagg HJ. Experimental and Clinical Studies on the Treatment of Cancer by dichlorethylsulphide (mustard gas). Ann Surg. 1931;93(1):190-9. [Link] [DOI:10.1097/00000658-193101000-00026] [PMID] [PMCID]
49. Balali‐Mood M, Hefazi M. Comparison of early and late toxic effects of sulfur mustard in Iranian veterans. Basic Clin Pharm Toxicol. 2006;99(4):273-82. [Link] [DOI:10.1111/j.1742-7843.2006.pto_429.x] [PMID]
50. Ahmadi K, Reshadatjoo M, Karami GR. Comparison of depression, anxiety and stress rate between chemical warfare victims and healthy persons in Sardasht, Iran. J Babol Univ Med Sci. 2010;12(1):44-50. [Persian] [Link]
51. Hosseini SH, Yaghoobi R, Haghdoost F, Dooshan A, Javedani Yekta S. Investigating the relationship between sleep quality and mental health in chemical veterans in comparison with their spouses and a control group. Int J Clin Med. 2014;5(4):162-6. [Link] [DOI:10.4236/ijcm.2014.54028]
52. Saeed KB, Parandeh A, Alhani F, Salaree MM. Health-related quality of life of chemical warfare victims: An assessment with the use of a specific tool. Trauma Mon. 2014;19(1):13800. [Link] [DOI:10.5812/traumamon.13800] [PMID] [PMCID]
53. Jones PW, Quirk FH, Baveystock CM. The saint George's respiratory questionnaire. Respir Med. 1991;85:25-31. [Link] [DOI:10.1016/S0954-6111(06)80166-6]
54. Abbasi M, Jamali HA, Omidi Oskouei AR. Quality of life of chemically-disabled war veterans involved in pulmonary complications of sulfur mustard gas in Sardasht. Qom Univ Med Sci J. 2012;5(4):34-9. [Persian] [Link]
55. Panahi Y, Davoodi SM, Naghizadeh MM. Dermatology related quality of life in sulfur mustard exposed veterans. Int J Behav Sci. 2008;2(3):237-44. [Persian] [Link]
56. Panahi Y, Davoudi SM, Sadr SB, Naghizadeh MM, Mohammadi-Mofrad M. Impact of pruritus on quality of life in sulfur mustard-exposed Iranian veterans. Int J Dermatol. 2008;47(6):557-61. [Link] [DOI:10.1111/j.1365-4632.2008.03650.x] [PMID]