
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

1.0
Cite Score 2025
SJR: 0.129 / SNIP: 0.140
Volume 16, Issue 3 (2024)
Iran J War Public Health 2024, 16(3): 261-267 |
Back to browse issues page
Article Type:
Subject:






Ethics code: IR.SSRC.REC.1400.093
History
Received: 2024/09/21 | Accepted: 2024/11/6 | Published: 2024/11/12
Received: 2024/09/21 | Accepted: 2024/11/6 | Published: 2024/11/12
How to cite this article
Ahar S, Samadi H, Barzegari Marvast H, Hajlotfalian M. Impact of Exercise and Virtual Reality on Psychomotor Skills in Post-Traumatic Stress Disorder Affected Armed Forces Personnel. Iran J War Public Health 2024; 16 (3) :261-267
URL: http://ijwph.ir/article-1-1508-en.html
URL: http://ijwph.ir/article-1-1508-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Department of Physical Education and Sports Sci¬ence, Faculty of Psychology and Educational Sciences, Yazd University, Yazd, Iran
Full-Text (HTML) (1116 Views)
Introduction
Post-Traumatic Stress Disorder (PTSD), formerly known as "war-related psychiatric disorders", is a significant and incapacitating mental health condition that arises following exposure to a traumatic event or the recollection and re-experiencing of such an event [1]. Following the onset of post-traumatic stress disorder (PTSD), individuals exhibit pronounced clinical symptoms that are linked to significant adverse effects on both mental and physical health, as well as a substantial decline in overall quality of life [2]. Recent studies have pointed to an increased risk of PTSD among military personnel dealing with daily high-stress situations, particularly those facing wartime conditions [3, 4]. Platania et al. demonstrated in their study that the risk of exposure to PTSD increases among military personnel who encounter severe stress-inducing events [5].
The prevalence of post-traumatic stress disorder varies significantly worldwide [6, 7]. The current estimate in the United States suggests that 6 to 8% of adults aged 18 or older live with this disorder, with active U.S. military personnel facing rates 2 to 3 times higher [3, 7]. In Iran, there are no exact statistics of those suffering from this disorder among the warriors returning from the war or other military personnel, but some studies have mentioned its prevalence between 20 and 30% [8].
Multiple studies demonstrate that the persistence of post-traumatic stress disorder leads to several physiological and biological consequences, including reduced sensory function (vision, vestibular, proprioception), motor function (strength, coordination, endurance) and integration (response time, the ability to do several tasks) which can lead to accelerated decline in performance and as a result impaired functional balance, motor coordination and muscle weakness at the end of life [9]. Motor coordination and function are closely interconnected and play a key role in physical-motor fitness, thereby influencing various aspects of quality of life [10]. Quality of life personal beliefs, and social interaction [11]. Post-traumatic stress disorder directly influences all aspects of quality of life by reducing physical, psychological, and social functioning, potentially hindering individuals from conducting daily activities across diverse life domains [12]. Encompasses various dimensions such as physical health and mental well-being.
Recognizing the significance of enhancing psychomotor components in individuals with PTSD, particularly within the military, there exists contradictory findings regarding the effectiveness of different treatment protocols [7, 13]. Non-pharmacological approaches, such as regular participation in physical activity programs, represent one avenue to promote both physical and cognitive health [14, 15].
Moreover, the benefits of physical activity extend to inactive elderly women, with meditation, yoga, rhythmic movements, and aerobics proven to decrease depression levels and elevate quality of life [16]. Pilates is an emerging mind-body exercise emphasizing precise control, posture, and breathing. With its focus on body-mind coordination and attention to balance and posture control, Pilates presents a valuable intervention for enhancing psychomotor components in individuals [17].
Various studies have demonstrated the effectiveness of these exercises in improving postural control, muscular strength, motor coordination, and quality of life factors. For instance, an improvement in the quality of life of patients with spondylolysis was reported after 8 weeks of Pilates training [18]. Additionally, researchers have noted enhancements in balance and motor coordination, along with reductions in anxiety, depression, and fatigue, as well as an increase in quality of life and vitality following 6 weeks of Pilates exercises [19].
On the other hand, in recent years, the use of virtual reality exercises (exergame) for the rehabilitation of patients is one of the scientific fields that has attracted the attention of researchers [20]. Exergame is a type of virtual reality and a new technology that allows a person to interact with a simulated computer environment. In this method, a person can perform the tasks asked of him in the virtual environment in a real environment and evaluate and correct his performance through instant feedback received from the virtual environment and also predict the events of the environment. And react appropriately to them. Exergame has become a cheap and reliable program to implement and improve health programs, balance and control neuromuscular coordination [21]. Castelli supported the positive effects of video game rehabilitation on balance and mobility and psychological factors (stress, anxiety) of people with MS [22]. However, what has not been addressed so far is the effects of these interventions on soldiers suffering from PTSD, and the results of this research, in addition to providing evidence in the field of improving the quality of life and reducing the problems of these people, can be used as an effective program and at the same time, it is pleasant to be introduced along with other treatment and rehabilitation protocols.
The integration of Pilates and exergame exercises, characterized by their varied and targeted movements, presents a promising alternative for enhancing physical activity participation within the community, particularly among military personnel. Given the limited historical context regarding the efficacy of Pilates and exergame exercises on psychomotor components, there is a pressing need to advocate for these modalities and establish a framework to promote their utilization, particularly among armed forces personnel. Thus, this study seeks to explore the effects of Pilates and exergame exercise interventions on the psychomotor components of military personnel diagnosed with post-traumatic stress disorder (PTSD).
Materials and Methods
The research approach utilized a practical, semi-experimental method, implementing a pre-test-post-test design with two experimental groups and a control group.
Statistical population and sample size
The study examined a statistical sample of male armed forces personnel diagnosed with post-traumatic stress disorder (PTSD) who sought treatment from recognized psychological centers. The sample size was calculated using the formula below, assigning 20 individuals to each group, with a Type I error rate of 0.05 [23].

A total of 60 participants were selected purposefully from specialized centers in Yazd. Participants met specific inclusion criteria, including being male armed forces employees aged 30-55 years, with no recent lower limb fractures, not using walking aids, and free from significant visual, hearing, or cognitive impairments. Further criteria required the absence of other neurological diseases, avoidance of concurrent psychological treatments, and validation through a demographic form and expert evaluation.
Exclusion criteria included non-participation during evaluation or intervention sessions, missing more than two consecutive sessions, failing to meet entry requirements such as maintaining regular sleep patterns and abstaining from substance use, and withdrawal of consent. To ensure adherence, participant reports were regularly reviewed throughout the project to confirm their continued eligibility and participation.
Data collection tools
1. Personal information form: This researcher-developed form collected details such as age, weight, height, gender, education level, and any physical or cognitive ailments.
2. Informed consent form for research participation: This document detailed the study's objectives and methodology, ensuring participants understood that no specific physical or psychological harm would occur. It highlighted their right to withdraw at any time and guaranteed the confidentiality of their information.
3. Quality of life questionnaire: The SF-36 questionnaire was used to assess quality of life across physical and psychological domains. It includes 36 items categorized into eight subscales, such as physical functioning, bodily pain, general health, and mental well-being [24]. Its validity and reliability in Iran were previously established by Montazeri et al., with subscale reliability coefficients ranging from 0.77 to 0.95 [25].
4. Functional balance: Functional balance was assessed using the Balance Scale Test, considered the gold standard for such evaluations. This test includes 14 tasks, such as standing with and without support and transitioning from sitting to standing. Each task is scored from 0 to 4, with a maximum possible score of 56 [26]. Its validity and reliability in Iran were confirmed by Salavati et al. [27].
5. Motor coordination: Motor coordination was evaluated using the Tandem Gait Coordination Test, which involves walking in a straight line heel-to-toe for up to 15 steps. The score reflects the number of steps completed before deviating from the path, with a maximum score of 15. The test's reliability and validity were confirmed in local studies [28].
Implementation method
The study was conducted in 2023 after receiving ethical approval from the Ethics Committee of the Sport Sciences Research Institute. Participants were randomly assigned to one of three groups: a Pilates exercise group (20 participants), a virtual reality exergame group (20 participants), and a control group (20 participants). Both experimental groups underwent their interventions for eight weeks, with three one-hour sessions per week, while the control group continued their usual daily routines and treatments.
According to the Pilates exercise protocol [29], the intervention was carried out in four progressive stages: the first two weeks involved mat-based exercises, followed by two weeks of exercises incorporating an aerobic ball. The third stage, during weeks five and six, introduced light weights and resistance bands, while the final two weeks combined movements from all previous stages. The exercises were designed to progress in intensity and complexity over time. Conversely, the virtual reality group engaged in sports-based activities using specialized Xbox Kinect 360 software, including boxing, table tennis, football, golf, and American football. Participants received training in the virtual reality tasks before the intervention, with each session structured to include warm-up exercises, core activities, and cooldown periods, all conducted over eight weeks.
Descriptive statistics, including mean, standard deviation, and other central tendency measures, were used to summarize the collected data. The study employed multivariate analysis of variance (MANOVA) to evaluate and compare the effectiveness of Pilates and virtual reality exercises on psychological outcomes, specifically quality of life, and motor outcomes, such as functional balance and motor coordination. The Bonferroni post hoc test was applied to identify specific differences between groups. Statistical analysis was conducted using SPSS version 25, with a significance level of 0.05.
Prior to multivariate covariance analysis (MANCOVA), assumptions were verified. The Shapiro-Wilk and Kolmogorov-Smirnov tests confirmed that the quality of life variable as a psychological component and the balance and motor coordination variables as motor components followed a normal distribution in both pre- and post-test stages (p<0.05). Levene's test indicated homogeneity of variances for quality of life (p=0.754, F=0.284), balance (p=0.350, F=3.544), and motor coordination (p=0.902, F=10.30). The M’box test confirmed the assumption of homogeneity of covariance matrices (p=0.069, F=1.40, Box's M=48.36). Thus, the conditions necessary for conducting MANCOVA were satisfied.
Findings
Demographic characteristics of the participants in 3 groups of 20 people were collected. The groups were relatively similar in demographics, with minor variations in age, height, weight, military service record, and disorder history, ensuring baseline comparability across the groups (Table 1).
Table 1. Descriptive values related to the demographic characteristics of research participants by group

Post-test results indicated improvements in quality of life, balance, and motor coordination for the sport training and exergame groups compared to the control group, with the sport training group showing the highest gains in quality of life and motor coordination (Table 2).
Table 2. Mean values, and standard deviation of the measured variables of the subjects by group in the pre-test and post-test stages

The results of the Wilks's lambda test from the set of multivariate tests showed that there was a significant difference between the experimental group of exercise training, exergame and control at least in the quality-of-life variable (p<0.01, F=14.201). The value of Wilks's lambda test for functional balance and motor coordination also confirmed a significant difference between the groups (p>0.01, F=23.770). According to the eta square, it can be stated that 76, 65 and 53% of the difference in quality-of-life scores, functional balance and movement coordination was the result of the difference in training methods (p<0.01; Table 3).
Table 3. Results of the multivariate covariance test to determine the difference in mean scores of variables in the pre-test & post-test

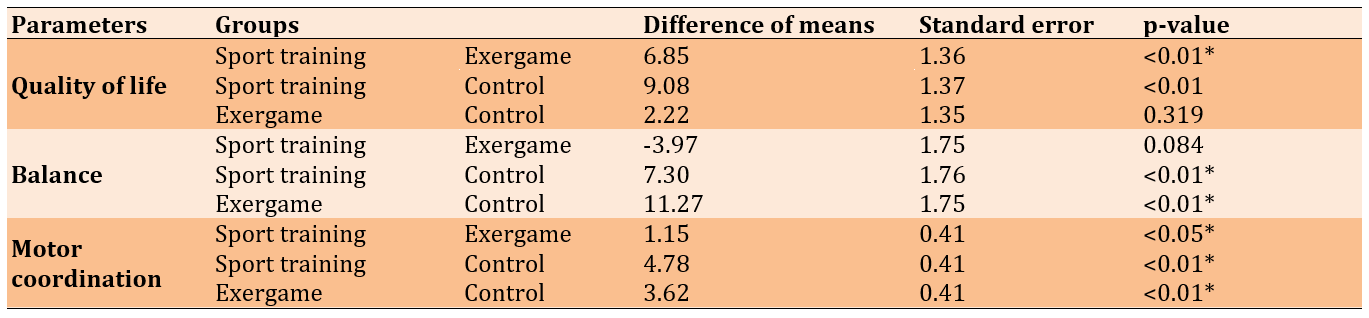
Bonferroni's post hoc test was used to determine the difference between the three groups (Table 4). It was determined that Pilates trainings significantly improved quality of life scores more than exergame intervention. There was no significant difference between the control and exergame groups. The group of virtual reality intervention (exergame) and Pilates had a significant difference compared to the control group, but no significant difference was observed between these two training methods. In the motor coordination variable, there was a significant difference between the two training methods of exergame and Pilates and between these two training methods and the control group (Table 4).
Table 4. Bonferroni's post hoc test results in order to pairwise compare the scores of the evaluated variables between the three research groups
Discussion
The objective of this study was to explore the impact of Pilates and virtual reality exercises on the various aspects of quality of life, functional balance, and motor coordination among military personnel diagnosed with post-traumatic stress disorder (PTSD). The findings showed that both types of activities significantly improved participants' quality of life. Specifically, the positive effects of Pilates on quality of life matched earlier research by Jamali Brayjani et al. [18], Akbaş & Ünver [19], and Jalali Aghdam et al. [30]. However, these results contrasted with those have reported by Hassani et al. [31]. Such differences might stem from variations in exercise types, intensities, intervention durations, and the lifestyles of the participants. Pilates not only boosts physical and mental well-being but also helps reduce depression, anxiety, and sleep issues. This, in turn, enhances individuals' abilities to perform daily tasks, make better decisions, feel more satisfied, and engage more effectively in their activities, leading to an overall better quality of life [19, 32]. Regarding the results of exergame on quality-of-life components, it's worth noting that this is a newer form of exercise that leverages computer technology and extensive data processing. Recent studies have been investigating how effective these activities are for various physical and mental health functions. Virtual reality games, in particular, offer a wide range of options and create interactive experiences that can improve patients' mental health while also enhancing their physiological well-being. A systematic review by Chuang et al. highlights a significant positive impact of virtual reality interventions on the mental health of those with psychological disorders [21]. The benefits of exergame can be explained by its ability to stimulate the release of dopamine, serotonin, and endorphins, which contribute to feelings of happiness and well-being [20, 21]. While the study found that both Pilates and exergame positively influenced the quality of life for military personnel with PTSD, Pilates proved to be more effective than exergame. This raises an important question; Should individuals concentrate on aerobic exercises to improve their capabilities, or would participating in structured sports be more beneficial? This topic certainly warrants further investigation.
The current study found that both Pilates exercises and virtual reality significantly enhanced functional balance and motor coordination in military personnel dealing with post-traumatic stress disorder (PTSD). This positive effect on balance is consistent with previous research. For instance, Yazdani et al. have showed that Pilates exercises effectively improved postural control in older women who had experienced falls [33]. Similarly, Mohammadi Arani & Rahnama have conducted an 8-week Pilates program for elderly women, revealing significant improvements in both static and dynamic balance [34]. The benefits of Pilates can be attributed to its ability to reduce visceral fat, which may help alleviate pain across different body areas and prevent injuries related to overuse or excessive strain on muscles. Additionally, improved balance can result from various neural adaptations that occur with training. These adaptations include using more efficient neural units, reorganizing the sensory-motor cortex, enhancing the effectiveness of synaptic connections, increasing overall nervous system activation, reducing inhibitory responses, and improving the transmission of impulses between neural pathways. All these factors contribute to better sensory processing and coordination [17, 30, 31]. The body operates as a kinetic chain, where every system and muscle group play an essential role. In this framework, strength, core stability, and balance are all interconnected [29, 35]. Also, research evidence shows that exergame interventions, as an attractive and enjoyable method, can increase the level of interaction and participation and adherence to the rehabilitation process in people [20, 21]. For instance, Khan Ghouri et al. have found out that virtual reality games positively affected balance and lower limb function in children with Down syndrome [36]. Similarly, Taheri et al. report that an eight-week program of virtual reality-based physical training significantly improved walking mechanics, muscle strength, and balance in women with multiple sclerosis [37]. One reason virtual reality games are seen as beneficial could be their ability to enhance blood flow in specific brain areas, like the superior temporal gyrus, which is important for balance. These virtual reality programs stimulate these regions, leading to changes in the brain's structure and function [20, 21]. Virtual reality offers several advantages, including the opportunity for repetitive practice in a fun and motivating environment, reduced fear of failure, the introduction of new games in each therapy session that gradually increase in complexity, and quick sensory feedback during gameplay. These features help create a training experience that closely resembles real-life situations [20, 21]. This study highlights how such interventions can positively impact functional balance, motor coordination, and overall quality of life for military personnel dealing with PTSD.
However, there were some limitations to this study. The sample included only male military personnel with PTSD, so we should be cautious about applying these results to other groups. Additionally, the research relied on convenience sampling and did not include follow-up assessments of the interventions. Given the limited research on PTSD in military settings, future studies should aim to address these limitations and explore additional psychological and motor factors. It is suggested that these training programs be incorporated alongside other activities for military members, especially for those dealing with PTSD.
Conclusion
Exercise and virtual reality training significantly improve the psychomotor skills of military personnel suffering from post-traumatic stress disorder (PTSD).
Acknowledgments: We would like to thank all the participants for their collaboration with the research team.
Ethical Permissions: This study received ethical approval from the Ethics Committee of the Sport Sciences Research Institute (IR.SSRC.REC.1400.093.). All participants were required to provide written informed consent prior to commencing any study procedures. Furthermore, the study was conducted meticulously in accordance with the ethical principles outlined in the Declaration of Helsinki.
Conflicts of Interests: The authors reported no conflicts of interests.
Authors' Contribution: Ahar S (First Author), Main Researcher/Statistical Analyst (50%); Samadi H (Second Author), Introduction Writer (17%); Barzegari Marvast H (Third Author), Methodologist/Discussion Writer (17%); Hajlotfalian M (Forth Author), Assistant Researcher (16%)
Funding/Support: The present study was not financially supported.
Post-Traumatic Stress Disorder (PTSD), formerly known as "war-related psychiatric disorders", is a significant and incapacitating mental health condition that arises following exposure to a traumatic event or the recollection and re-experiencing of such an event [1]. Following the onset of post-traumatic stress disorder (PTSD), individuals exhibit pronounced clinical symptoms that are linked to significant adverse effects on both mental and physical health, as well as a substantial decline in overall quality of life [2]. Recent studies have pointed to an increased risk of PTSD among military personnel dealing with daily high-stress situations, particularly those facing wartime conditions [3, 4]. Platania et al. demonstrated in their study that the risk of exposure to PTSD increases among military personnel who encounter severe stress-inducing events [5].
The prevalence of post-traumatic stress disorder varies significantly worldwide [6, 7]. The current estimate in the United States suggests that 6 to 8% of adults aged 18 or older live with this disorder, with active U.S. military personnel facing rates 2 to 3 times higher [3, 7]. In Iran, there are no exact statistics of those suffering from this disorder among the warriors returning from the war or other military personnel, but some studies have mentioned its prevalence between 20 and 30% [8].
Multiple studies demonstrate that the persistence of post-traumatic stress disorder leads to several physiological and biological consequences, including reduced sensory function (vision, vestibular, proprioception), motor function (strength, coordination, endurance) and integration (response time, the ability to do several tasks) which can lead to accelerated decline in performance and as a result impaired functional balance, motor coordination and muscle weakness at the end of life [9]. Motor coordination and function are closely interconnected and play a key role in physical-motor fitness, thereby influencing various aspects of quality of life [10]. Quality of life personal beliefs, and social interaction [11]. Post-traumatic stress disorder directly influences all aspects of quality of life by reducing physical, psychological, and social functioning, potentially hindering individuals from conducting daily activities across diverse life domains [12]. Encompasses various dimensions such as physical health and mental well-being.
Recognizing the significance of enhancing psychomotor components in individuals with PTSD, particularly within the military, there exists contradictory findings regarding the effectiveness of different treatment protocols [7, 13]. Non-pharmacological approaches, such as regular participation in physical activity programs, represent one avenue to promote both physical and cognitive health [14, 15].
Moreover, the benefits of physical activity extend to inactive elderly women, with meditation, yoga, rhythmic movements, and aerobics proven to decrease depression levels and elevate quality of life [16]. Pilates is an emerging mind-body exercise emphasizing precise control, posture, and breathing. With its focus on body-mind coordination and attention to balance and posture control, Pilates presents a valuable intervention for enhancing psychomotor components in individuals [17].
Various studies have demonstrated the effectiveness of these exercises in improving postural control, muscular strength, motor coordination, and quality of life factors. For instance, an improvement in the quality of life of patients with spondylolysis was reported after 8 weeks of Pilates training [18]. Additionally, researchers have noted enhancements in balance and motor coordination, along with reductions in anxiety, depression, and fatigue, as well as an increase in quality of life and vitality following 6 weeks of Pilates exercises [19].
On the other hand, in recent years, the use of virtual reality exercises (exergame) for the rehabilitation of patients is one of the scientific fields that has attracted the attention of researchers [20]. Exergame is a type of virtual reality and a new technology that allows a person to interact with a simulated computer environment. In this method, a person can perform the tasks asked of him in the virtual environment in a real environment and evaluate and correct his performance through instant feedback received from the virtual environment and also predict the events of the environment. And react appropriately to them. Exergame has become a cheap and reliable program to implement and improve health programs, balance and control neuromuscular coordination [21]. Castelli supported the positive effects of video game rehabilitation on balance and mobility and psychological factors (stress, anxiety) of people with MS [22]. However, what has not been addressed so far is the effects of these interventions on soldiers suffering from PTSD, and the results of this research, in addition to providing evidence in the field of improving the quality of life and reducing the problems of these people, can be used as an effective program and at the same time, it is pleasant to be introduced along with other treatment and rehabilitation protocols.
The integration of Pilates and exergame exercises, characterized by their varied and targeted movements, presents a promising alternative for enhancing physical activity participation within the community, particularly among military personnel. Given the limited historical context regarding the efficacy of Pilates and exergame exercises on psychomotor components, there is a pressing need to advocate for these modalities and establish a framework to promote their utilization, particularly among armed forces personnel. Thus, this study seeks to explore the effects of Pilates and exergame exercise interventions on the psychomotor components of military personnel diagnosed with post-traumatic stress disorder (PTSD).
Materials and Methods
The research approach utilized a practical, semi-experimental method, implementing a pre-test-post-test design with two experimental groups and a control group.
Statistical population and sample size
The study examined a statistical sample of male armed forces personnel diagnosed with post-traumatic stress disorder (PTSD) who sought treatment from recognized psychological centers. The sample size was calculated using the formula below, assigning 20 individuals to each group, with a Type I error rate of 0.05 [23].
A total of 60 participants were selected purposefully from specialized centers in Yazd. Participants met specific inclusion criteria, including being male armed forces employees aged 30-55 years, with no recent lower limb fractures, not using walking aids, and free from significant visual, hearing, or cognitive impairments. Further criteria required the absence of other neurological diseases, avoidance of concurrent psychological treatments, and validation through a demographic form and expert evaluation.
Exclusion criteria included non-participation during evaluation or intervention sessions, missing more than two consecutive sessions, failing to meet entry requirements such as maintaining regular sleep patterns and abstaining from substance use, and withdrawal of consent. To ensure adherence, participant reports were regularly reviewed throughout the project to confirm their continued eligibility and participation.
Data collection tools
1. Personal information form: This researcher-developed form collected details such as age, weight, height, gender, education level, and any physical or cognitive ailments.
2. Informed consent form for research participation: This document detailed the study's objectives and methodology, ensuring participants understood that no specific physical or psychological harm would occur. It highlighted their right to withdraw at any time and guaranteed the confidentiality of their information.
3. Quality of life questionnaire: The SF-36 questionnaire was used to assess quality of life across physical and psychological domains. It includes 36 items categorized into eight subscales, such as physical functioning, bodily pain, general health, and mental well-being [24]. Its validity and reliability in Iran were previously established by Montazeri et al., with subscale reliability coefficients ranging from 0.77 to 0.95 [25].
4. Functional balance: Functional balance was assessed using the Balance Scale Test, considered the gold standard for such evaluations. This test includes 14 tasks, such as standing with and without support and transitioning from sitting to standing. Each task is scored from 0 to 4, with a maximum possible score of 56 [26]. Its validity and reliability in Iran were confirmed by Salavati et al. [27].
5. Motor coordination: Motor coordination was evaluated using the Tandem Gait Coordination Test, which involves walking in a straight line heel-to-toe for up to 15 steps. The score reflects the number of steps completed before deviating from the path, with a maximum score of 15. The test's reliability and validity were confirmed in local studies [28].
Implementation method
The study was conducted in 2023 after receiving ethical approval from the Ethics Committee of the Sport Sciences Research Institute. Participants were randomly assigned to one of three groups: a Pilates exercise group (20 participants), a virtual reality exergame group (20 participants), and a control group (20 participants). Both experimental groups underwent their interventions for eight weeks, with three one-hour sessions per week, while the control group continued their usual daily routines and treatments.
According to the Pilates exercise protocol [29], the intervention was carried out in four progressive stages: the first two weeks involved mat-based exercises, followed by two weeks of exercises incorporating an aerobic ball. The third stage, during weeks five and six, introduced light weights and resistance bands, while the final two weeks combined movements from all previous stages. The exercises were designed to progress in intensity and complexity over time. Conversely, the virtual reality group engaged in sports-based activities using specialized Xbox Kinect 360 software, including boxing, table tennis, football, golf, and American football. Participants received training in the virtual reality tasks before the intervention, with each session structured to include warm-up exercises, core activities, and cooldown periods, all conducted over eight weeks.
Descriptive statistics, including mean, standard deviation, and other central tendency measures, were used to summarize the collected data. The study employed multivariate analysis of variance (MANOVA) to evaluate and compare the effectiveness of Pilates and virtual reality exercises on psychological outcomes, specifically quality of life, and motor outcomes, such as functional balance and motor coordination. The Bonferroni post hoc test was applied to identify specific differences between groups. Statistical analysis was conducted using SPSS version 25, with a significance level of 0.05.
Prior to multivariate covariance analysis (MANCOVA), assumptions were verified. The Shapiro-Wilk and Kolmogorov-Smirnov tests confirmed that the quality of life variable as a psychological component and the balance and motor coordination variables as motor components followed a normal distribution in both pre- and post-test stages (p<0.05). Levene's test indicated homogeneity of variances for quality of life (p=0.754, F=0.284), balance (p=0.350, F=3.544), and motor coordination (p=0.902, F=10.30). The M’box test confirmed the assumption of homogeneity of covariance matrices (p=0.069, F=1.40, Box's M=48.36). Thus, the conditions necessary for conducting MANCOVA were satisfied.
Findings
Demographic characteristics of the participants in 3 groups of 20 people were collected. The groups were relatively similar in demographics, with minor variations in age, height, weight, military service record, and disorder history, ensuring baseline comparability across the groups (Table 1).
Table 1. Descriptive values related to the demographic characteristics of research participants by group
Post-test results indicated improvements in quality of life, balance, and motor coordination for the sport training and exergame groups compared to the control group, with the sport training group showing the highest gains in quality of life and motor coordination (Table 2).
Table 2. Mean values, and standard deviation of the measured variables of the subjects by group in the pre-test and post-test stages
The results of the Wilks's lambda test from the set of multivariate tests showed that there was a significant difference between the experimental group of exercise training, exergame and control at least in the quality-of-life variable (p<0.01, F=14.201). The value of Wilks's lambda test for functional balance and motor coordination also confirmed a significant difference between the groups (p>0.01, F=23.770). According to the eta square, it can be stated that 76, 65 and 53% of the difference in quality-of-life scores, functional balance and movement coordination was the result of the difference in training methods (p<0.01; Table 3).
Table 3. Results of the multivariate covariance test to determine the difference in mean scores of variables in the pre-test & post-test
Bonferroni's post hoc test was used to determine the difference between the three groups (Table 4). It was determined that Pilates trainings significantly improved quality of life scores more than exergame intervention. There was no significant difference between the control and exergame groups. The group of virtual reality intervention (exergame) and Pilates had a significant difference compared to the control group, but no significant difference was observed between these two training methods. In the motor coordination variable, there was a significant difference between the two training methods of exergame and Pilates and between these two training methods and the control group (Table 4).
Table 4. Bonferroni's post hoc test results in order to pairwise compare the scores of the evaluated variables between the three research groups
Discussion
The objective of this study was to explore the impact of Pilates and virtual reality exercises on the various aspects of quality of life, functional balance, and motor coordination among military personnel diagnosed with post-traumatic stress disorder (PTSD). The findings showed that both types of activities significantly improved participants' quality of life. Specifically, the positive effects of Pilates on quality of life matched earlier research by Jamali Brayjani et al. [18], Akbaş & Ünver [19], and Jalali Aghdam et al. [30]. However, these results contrasted with those have reported by Hassani et al. [31]. Such differences might stem from variations in exercise types, intensities, intervention durations, and the lifestyles of the participants. Pilates not only boosts physical and mental well-being but also helps reduce depression, anxiety, and sleep issues. This, in turn, enhances individuals' abilities to perform daily tasks, make better decisions, feel more satisfied, and engage more effectively in their activities, leading to an overall better quality of life [19, 32]. Regarding the results of exergame on quality-of-life components, it's worth noting that this is a newer form of exercise that leverages computer technology and extensive data processing. Recent studies have been investigating how effective these activities are for various physical and mental health functions. Virtual reality games, in particular, offer a wide range of options and create interactive experiences that can improve patients' mental health while also enhancing their physiological well-being. A systematic review by Chuang et al. highlights a significant positive impact of virtual reality interventions on the mental health of those with psychological disorders [21]. The benefits of exergame can be explained by its ability to stimulate the release of dopamine, serotonin, and endorphins, which contribute to feelings of happiness and well-being [20, 21]. While the study found that both Pilates and exergame positively influenced the quality of life for military personnel with PTSD, Pilates proved to be more effective than exergame. This raises an important question; Should individuals concentrate on aerobic exercises to improve their capabilities, or would participating in structured sports be more beneficial? This topic certainly warrants further investigation.
The current study found that both Pilates exercises and virtual reality significantly enhanced functional balance and motor coordination in military personnel dealing with post-traumatic stress disorder (PTSD). This positive effect on balance is consistent with previous research. For instance, Yazdani et al. have showed that Pilates exercises effectively improved postural control in older women who had experienced falls [33]. Similarly, Mohammadi Arani & Rahnama have conducted an 8-week Pilates program for elderly women, revealing significant improvements in both static and dynamic balance [34]. The benefits of Pilates can be attributed to its ability to reduce visceral fat, which may help alleviate pain across different body areas and prevent injuries related to overuse or excessive strain on muscles. Additionally, improved balance can result from various neural adaptations that occur with training. These adaptations include using more efficient neural units, reorganizing the sensory-motor cortex, enhancing the effectiveness of synaptic connections, increasing overall nervous system activation, reducing inhibitory responses, and improving the transmission of impulses between neural pathways. All these factors contribute to better sensory processing and coordination [17, 30, 31]. The body operates as a kinetic chain, where every system and muscle group play an essential role. In this framework, strength, core stability, and balance are all interconnected [29, 35]. Also, research evidence shows that exergame interventions, as an attractive and enjoyable method, can increase the level of interaction and participation and adherence to the rehabilitation process in people [20, 21]. For instance, Khan Ghouri et al. have found out that virtual reality games positively affected balance and lower limb function in children with Down syndrome [36]. Similarly, Taheri et al. report that an eight-week program of virtual reality-based physical training significantly improved walking mechanics, muscle strength, and balance in women with multiple sclerosis [37]. One reason virtual reality games are seen as beneficial could be their ability to enhance blood flow in specific brain areas, like the superior temporal gyrus, which is important for balance. These virtual reality programs stimulate these regions, leading to changes in the brain's structure and function [20, 21]. Virtual reality offers several advantages, including the opportunity for repetitive practice in a fun and motivating environment, reduced fear of failure, the introduction of new games in each therapy session that gradually increase in complexity, and quick sensory feedback during gameplay. These features help create a training experience that closely resembles real-life situations [20, 21]. This study highlights how such interventions can positively impact functional balance, motor coordination, and overall quality of life for military personnel dealing with PTSD.
However, there were some limitations to this study. The sample included only male military personnel with PTSD, so we should be cautious about applying these results to other groups. Additionally, the research relied on convenience sampling and did not include follow-up assessments of the interventions. Given the limited research on PTSD in military settings, future studies should aim to address these limitations and explore additional psychological and motor factors. It is suggested that these training programs be incorporated alongside other activities for military members, especially for those dealing with PTSD.
Conclusion
Exercise and virtual reality training significantly improve the psychomotor skills of military personnel suffering from post-traumatic stress disorder (PTSD).
Acknowledgments: We would like to thank all the participants for their collaboration with the research team.
Ethical Permissions: This study received ethical approval from the Ethics Committee of the Sport Sciences Research Institute (IR.SSRC.REC.1400.093.). All participants were required to provide written informed consent prior to commencing any study procedures. Furthermore, the study was conducted meticulously in accordance with the ethical principles outlined in the Declaration of Helsinki.
Conflicts of Interests: The authors reported no conflicts of interests.
Authors' Contribution: Ahar S (First Author), Main Researcher/Statistical Analyst (50%); Samadi H (Second Author), Introduction Writer (17%); Barzegari Marvast H (Third Author), Methodologist/Discussion Writer (17%); Hajlotfalian M (Forth Author), Assistant Researcher (16%)
Funding/Support: The present study was not financially supported.
Keywords:
References
1. Ressler KJ, Berretta S, Bolshakov VY, Rosso IM, Meloni EG, Rauch SL, et al. Post-traumatic stress disorder: Clinical and translational neuroscience from cells to circuits. Nat Rev Neurol. 2022;18(5):273-88. [Link] [DOI:10.1038/s41582-022-00635-8]
2. Hall KS, Morey MC, Beckham JC, Bosworth HB, Sloane R, Pieper CF, et al. Warrior wellness: A randomized controlled pilot trial of the effects of exercise on physical function and clinical health risk factors in older military veterans with PTSD. J Gerontol A Biol Sci Med Sci. 2020;75(11):2130-8. [Link] [DOI:10.1093/gerona/glz255]
3. Farr OM, Sloan DM, Keane TM, Mantzoros CS. Stress-and PTSD-associated obesity and metabolic dysfunction: A growing problem requiring further research and novel treatments. Metabolism. 2014;63(12):1463-8. [Link] [DOI:10.1016/j.metabol.2014.08.009]
4. Hall KS, Morey MC, Bosworth HB, Beckham JC, Pebole MM, Sloane R, et al. Pilot randomized controlled trial of exercise training for older veterans with PTSD. J Behav Med. 2020;43(4):648-59. [Link] [DOI:10.1007/s10865-019-00073-w]
5. Platania S, Castellano S, Petralia MC, Digrandi F, Coco M, Pizzo M, et al. The moderating effect of the dispositional resilience on the relationship between post-traumatic stress disorder and the professional quality of life of the military returning from the peacekeeping operations. Mediterr J Clin Psychol. 2020;8(3). [Link]
6. Atwoli L, Stein DJ, Koenen KC, McLaughlin KA. Epidemiology of posttraumatic stress disorder: Prevalence, correlates and consequences. Curr Opin Psychiatry. 2015;28(4):307-11. [Link] [DOI:10.1097/YCO.0000000000000167]
7. Whitworth JW, Ciccolo JT. Exercise and post-traumatic stress disorder in military veterans: A systematic review. Mil Med. 2016;181(9):953-60. [Link] [DOI:10.7205/MILMED-D-15-00488]
8. Mohaghegh-Motlagh SJ, Momtazi S, Musavi-Nasab SN, Arab A, Saburi E, Saburi A. Post-traumatic stress disorder in male chemical injured war veterans compared to non-chemical war veterans. Med J Mashhad Univ Med Sci. 2014;56(6):361-8. [Persian] [Link]
9. Katz-Leurer M, Rotem H, Keren O, Meyer S. Balance abilities and gait characteristics in post-traumatic brain injury, cerebral palsy and typically developed children. Dev Neurorehabil. 2009;12(2):100-5. [Link] [DOI:10.1080/17518420902800928]
10. Theofilou P. Quality of life: Definition and measurement. Eur J Psychol. 2013;9(1):150-62. [Link] [DOI:10.5964/ejop.v9i1.337]
11. Scoglio AA, Reilly ED, Girouard C, Quigley KS, Carnes S, Kelly MM. Social functioning in individuals with post-traumatic stress disorder: A systematic review. Trauma Violence Abuse. 2022;23(2):356-71. [Link] [DOI:10.1177/1524838020946800]
12. Oum SJ, Choi JH, Kim TY, Chung HG, Chung MY, So HS. The relationship between posttraumatic stress disorder and the quality of life among the Vietnam war veterans. Korean J Psychosom Med. 2011;19(2):83-91. [Link]
13. Samadi H, Moradi J, Karimi H. Effectiveness of sports activities on cognitive emotion regulation strategies, perceived psychological stress, and psychological hardiness of veterans and the disabled. Iran J War Public Health. 2022;14(1):43-9. [Link]
14. Moreira NB, Da Silva LP, Rodacki ALF. Aquatic exercise improves functional capacity, perceptual aspects, and quality of life in older adults with musculoskeletal disorders and risk of falling: A randomized controlled trial. Exp Gerontol. 2020;142:111135. [Link] [DOI:10.1016/j.exger.2020.111135]
15. Silva MR, Alberton CL, Portella EG, Nunes GN, Martin DG, Pinto SS. Water-based aerobic and combined training in elderly women: Effects on functional capacity and quality of life. Exp Gerontol. 2018;106:54-60. [Link] [DOI:10.1016/j.exger.2018.02.018]
16. Kim YH, Kim HJ, Do Ahn S, Seo YJ, Kim SH. Effects of meditation on anxiety, depression, fatigue, and quality of life of women undergoing radiation therapy for breast cancer. Complement Ther Med. 2013;21(4):379-87. [Link] [DOI:10.1016/j.ctim.2013.06.005]
17. Lim EJ, Hyun EJ. The impacts of Pilates and yoga on health-promoting behaviors and subjective health status. Int J Environ Res Public Health. 2021;18(7):3802. [Link] [DOI:10.3390/ijerph18073802]
18. Jamali Brayjani S, Rahnama N, Abrishamkar S. The effect of eight weeks Pilates exercises on pain and quality of life in patients with spondylolysis. PARS J Med Sci. 2019;17(1):33-41. [Persian] [Link] [DOI:10.52547/jmj.17.1.33]
19. Akbaş E, Ünver B. A six-week Pilates exercise protocol for improving physical and mental health-related parameters. Malays J Mov Health Exerc. 2018;7(2):65-79. [Link] [DOI:10.4103/2600-9404.323073]
20. Costa MTS, Vieira LP, De Oliveira Barbosa E, Oliveira LM, Maillot P, Vaghetti CAO, et al. Virtual reality-based exercise with exergames as medicine in different contexts: A short review. Clin Pract Epidemiol Ment Health. 2019;15:15-20. [Link] [DOI:10.2174/1745017901915010015]
21. Chuang CS, Chen YW, Zeng BY, Hung CM, Tu YK, Tai YC, et al. Effects of modern technology (exergame and virtual reality) assisted rehabilitation vs conventional rehabilitation in patients with Parkinson's disease: A network meta-analysis of randomised controlled trials. Physiotherapy. 2022;117:35-42. [Link] [DOI:10.1016/j.physio.2022.07.001]
22. Castelli L. Home-based exergames to improve cognitive function in Multiple Sclerosis: The EXTREMUS Study [dissertation]. Sardinia: The University of Cagliari; 2024. [Link]
23. Cochran WG, Mosteller F, Tukey JW. Principles of sampling. J Am Stat Assoc. 1954;49(265):13-35. [Link] [DOI:10.1080/01621459.1954.10501212]
24. Ware JE, Gandek B, IQOLA Project Group. The SF-36 health survey: Development and use in mental health research and the IQOLA Project. Int J Ment Health. 1994;23(2):49-73. [Link] [DOI:10.1080/00207411.1994.11449283]
25. Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The short form health survey (SF-36): Translation and validation study of the Iranian version. Qual Life Res. 2005;14(3):875-82. [Link] [DOI:10.1007/s11136-004-1014-5]
26. Muir SW, Berg K, Chesworth B, Speechley M. Use of the berg balance scale for predicting multiple falls in community-dwelling elderly people: A prospective study. Phys Ther. 2008;88(4):449-59. [Link] [DOI:10.2522/ptj.20070251]
27. Salavati M, Negahban H, Mazaheri M, Soleimanifar M, Hadadi M, Sefiddashti L, et al. The Persian version of the berg balance scale: Inter and intra-rater reliability and construct validity in elderly adults. Disabil Rehabil. 2012;34(20):1695-8. [Link] [DOI:10.3109/09638288.2012.660604]
28. James EG, Leveille SG, You T, Hausdorff JM, Travison T, Manor B, et al. Gait coordination impairment is associated with mobility in older adults. Exp Gerontol. 2016;80:12-6. [Link] [DOI:10.1016/j.exger.2016.04.009]
29. Liposcki DB, Da Silva Nagata IF, Silvano GA, Zanella K, Schneider RH. Influence of a Pilates exercise program on the quality of life of sedentary elderly people: A randomized clinical trial. J Bodyw Mov Ther. 2019;23(2):390-3. [Link] [DOI:10.1016/j.jbmt.2018.02.007]
30. Jalali Aghdam S, Mohammadzade H, Dehghanizade J. The effect of a course of Pilates exercises on serum BDNF levels, balance, and quality of life of menopausal and non-menopausal women. J Sports Mot Dev Learn. 2024;16(1):21-35. [Persian] [Link]
31. Hassani N, Heravi-Karimooi M, Rejeh N, Danesh Ashtiani MH, Sharifnia H, Ghanbari M, et al. The effect of Pilates exercise on quality of life of elderly women with type 2 diabetes. PAYESH. 2018;17(5):531-9. [Persian] [Link]
32. Fazlollazadeh N, Habibian M, Askari B. Effect of Pilates and Vitamin D supplementation on quality of life (QoL) and mental health of overweight men: A randomized clinical trial. J Arak Univ Med Sci. 2022;25(2):200-13. [Persian] [Link] [DOI:10.32598/jams.25.2.3537.7]
33. Yazdani S, Mojarradi R, Eskandarnejad M. The effect of selected Pilates exercises on the postural control and quality of life in older women with a history of falls. Mind Mov Behav. 2022;1(1):61-75. [Persian] [Link]
34. Mohammadi Arani M, Rahnama N. Comparison of the effect of training with balance board and Pilates and combined on the static and dynamic balance of elderly women. J Sport Exerc Physiol. 2021;14(1):21-30. [Persian] [Link] [DOI:10.52547/joeppa.14.1.21]
35. Surbala L, Khuman PR, Trivedi P, Devanshi B, Mital V. Pilates versus conventional balance training on functional balance and quality of life in elderly individuals: A randomized controlled study. Sch J Appl Med Sci. 2014;2(1B):221-6. [Link]
36. Khan Ghouri EUR, Memon AG, Ali S, Adnan Q, Tahir S. Effects of virtual reality on static and dynamic balance among individuals with down syndrome. J Liaquat Univ Med Health Sci. 2024;23(02):116-20. [Link] [DOI:10.22442/jlumhs.2024.01057]
37. Taheri S, Parvinpour S, Balali M. The effect of eight weeks of virtual reality-based physical training on kinematic indicators of gait, muscle strength, and balance in women with Multiple Sclerosis. J Adv Cogn Sci. 2022;24(3):1-16. [Persian] [Link]