
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

1.0
Cite Score 2025
SJR: 0.129 / SNIP: 0.140
Volume 15, Issue 4 (2023)
Iran J War Public Health 2023, 15(4): 395-403 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2023/10/31 | Accepted: 2024/01/2 | Published: 2024/01/25
Received: 2023/10/31 | Accepted: 2024/01/2 | Published: 2024/01/25
How to cite this article
Özmen O, Özmen P. A Scientific Evaluation for Military Medical Services in the Russia-Ukraine War. Iran J War Public Health 2023; 15 (4) :395-403
URL: http://ijwph.ir/article-1-1409-en.html
URL: http://ijwph.ir/article-1-1409-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:


1- Istanbul Okan University, Ankara, Türkiye
2- Ministry of National Defense of Republic of Türkiye
2- Ministry of National Defense of Republic of Türkiye
Full-Text (HTML) (2455 Views)
Introduction
Despite there being many terrorist groups and their attacks throughout the world, we have to put forward new ideas and approaches to international hybrid warfare in terms of medical delivery systems because of the comparisons and contrasts between terrorist attacks and hybrid international wars. We know that states resort to hybrid war to circumvent existing rules of law within the scope of the use of force [1]. The best and most innovative way to do this seems to be to examine the ongoing Russia-Ukraine war regarding health delivery services, in which both national armies have their own military medical structures and systems.
This article aims to show differences in terms of the medical delivery system between new hybrid national military conflicts and classic conventional war and/or terrorist conflicts and to propose new ideas and approaches in medical preparation to challenge adversaries.
However, to evaluate medical situations in warfare, you need to go and see the battlefield as an observer. However, it is impossible to stay on the battlefield as an impartial observer in wars of the modern age because of concerns about risks to the military intelligence of parties. Instead, if you want to evaluate relying on open sources, you have to regard bilateral ideas, bias, and cheating in official media, social media, and cyberspace.
In January 2022, it was observed that Ukraine’s Field Hospitals had been moved along the northern, eastern, and southeastern borders by the International Community. “Hospitals’ movement is the circumstantial evidence of about the bloody war and commander intent”, according to Napoleon (1763-1821) [2]. The claim is that hospitals were targeted by Russian forces from the borderline to the deep of the country. Zhytomyr Hospital is deployed as far west as 400km. From the borderline, it was targeted by Russia. According to the news, attacks targeted hospitals, energy, and water sources in war. Russian missiles can reach Ukraine's western, up to 20km from the Polish border. This means that the entire Ukraine is considered to be under Russian missile influence [3]. According to some reports, red cross emblems and international consensus on humanitarian treatments don’t provide protection in Ukraine. Moreover, some car parks and basements have been used as medical facilities [2]. According to paper sources, attacks targeted hospitals, electricity, and other energy sources in Ukraine and increased HIV/AIDS, Tuberculosis, and COVID-19 prevalences in cities [4]. In addition, notwithstanding continued studies on blood transfusion in Ukraine ever during the war, these activities have been undermined by aggressions of war [5] and affect the circumstances of wounded on the battlefield. Countries such as Poland, where most Ukrainian refugees initially migrated, helped Ukraine close the gaps in the health infrastructure that collapsed due to the war and shouldered the burden of health services, especially child immunizations, COVID-19 vaccines, and chronic disease treatments [6].
The war has adversely affected chronic patients and their treatments. Cancer patients are the group who are the most affected deeply. The reasons for adverse effects on chronic illnesses like cancers during the war are damage to the healthcare infrastructure and patient displacement. The war has interrupted both treatments and trials on cancer in both Russia and Ukraine [7]. Similarly, patients with rheumatological disorders and rheumatologists had to leave the city and country due to war effects [8]. Although telemedicine is considered a way for patients with chronic diseases, district access to the internet and limited medicine and drug logistic services are a great problem in war times.
President “Putin” has claimed that "The USA and NATO are rapidly deploying their secret biological laboratories close to Russian borders and preparing Ukraine for a big war." he said that “Ukraine has attacked the Russian people since 2014 starting from Donbas” [9]. Russia also blames Ukraine for crimes against humanity, just like Ukraine and its allies do.
Despite the Ministry of Defense of the Russian Federation’s official journal claims of opposition, according to “Military Industry Courier,” which is a military journal published in Russia, the military medical system on the battlefield is the restricting adverse factor for the military capacity of the Russian Army [10]. In 2018, it was claimed that thanks to developed measures, patient volume decreased among soldiers, an effective medevac system by airway, a telemedicine system, and a medical and psychological rehabilitation system for the army in Russia. Moreover, it had been claimed that in Kirov Military Medical Academy, capacity had been increased 8 times, 20.000 surgeries per year, 16.000 of them were complex and high technology surgeries, and a multidisciplined clinic had been set up for war injured in the academy, recently [11]. However, military strategists had predicted in 2018 that Bryansk, Orel, Kursk, and Belgorod Military Hospitals, part of the military healthcare system, would remain on the battlefield when war broke out on the Ukrainian border. This situation brought about extreme workload in poor war circumstances because of their deploy area. These hospitals had been deployed in the military, humanity, medical logistics, evacuation routes, and target routes for airstrikes by adversaries. Moreover, this route was capable of war fugitives and immigrants as well as civilians adversely affected by the war. These circumstances increased the workload of these military medical facilities, and they were near to targeting adversaries’ artillery and rocket attacks.
Besides the adverse effects of war on emergency healthcare and clinic systems, cyberattacks on healthcare are a problem nowadays. Although it was not brought to the agenda for the Russia-Ukraine war, it is known that there were 679 cyberattacks on healthcare services in the USA in 2021. This type of attack is a hybrid warfare component usually carried out by criminal hackers. This type of attack is a hybrid warfare component usually carried out by criminal hackers. These attacks targeted booking systems, medical technologic diagnostic systems, and patient records [12].
Food security, environmental pollution, increased violent behaviors by which damage to the social system, disruption of the education system, and freshwater security should be considered as components that threaten the healthcare system indirectly caused by the conflicts between Russia and Ukraine, like in every war [13].
Information and Methods
In this study, scientific literature was searched limited to 2017-2023 for “Trdizin”, and limited to 2022-2023 for “Google Scholar” and “Elsevier”, the last 5 years for “PubMed”, on military healthcare services during the Ukraine-Russia war. We have considered only published papers in peer-reviewed journals using main terms such as “Medical Services in Ukraine-Russia War” and ”Combat Casualty in Ukraine-Russia War”. Terms “injury, military, medicine, wounded, medevac” were used as secondary expressions for search in literature.
Table 1. List of Studied Articles
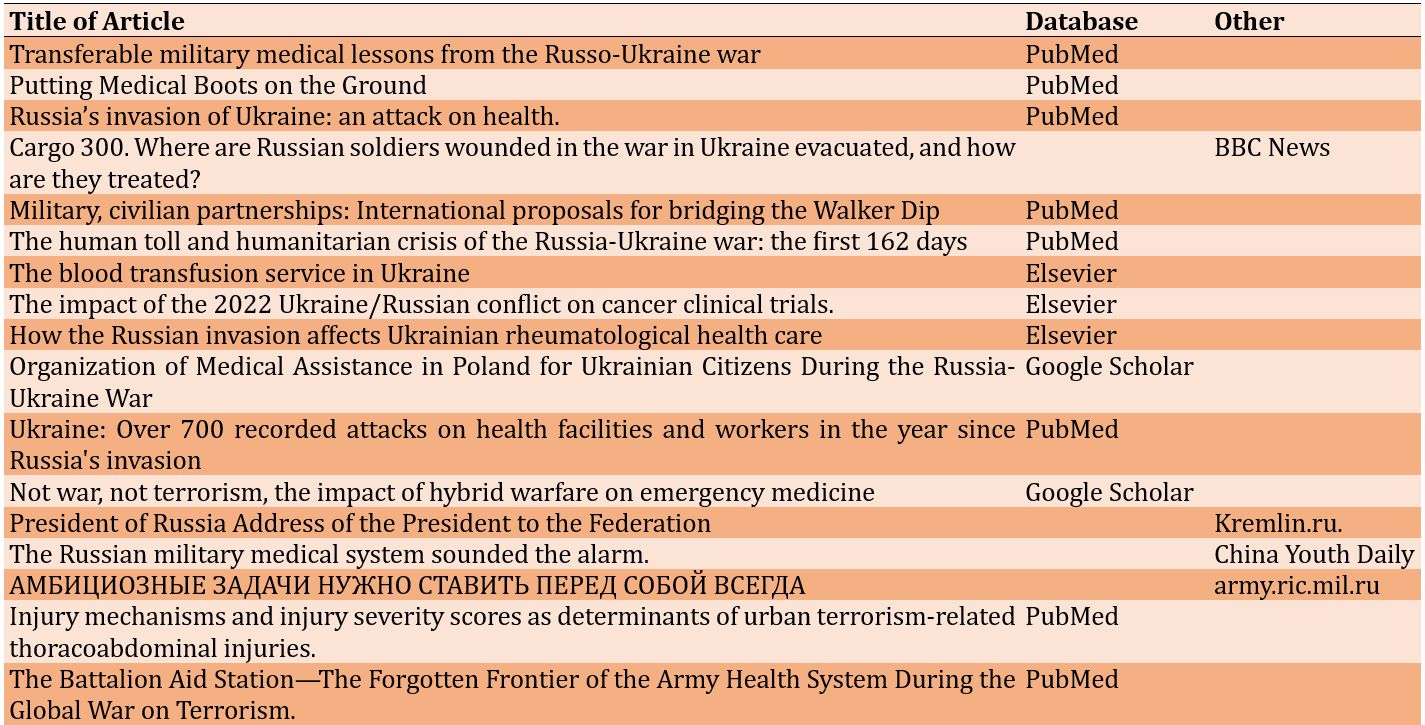
Furthermore, we have searched the military medical literature and news from China, Iran, the United Kingdom, Belarus, and the United States, considering the deception, secrecy, and the use of the media principles of war. We used the English language for all scientific literature searching, but for news, we used the Google Translate application to translate from Chinese, Persian, and Russian to English.
We confirmed all the information we obtained by comparing the official sites of governmental and nongovernmental corporations, and we highlighted some of the information we found suspicious in the article. World Health Organization database, OECD database, European :union: database, and official websites of the Ministries of Defense of both states have been used for official demographic information, including wounded and died numbers, types of casualties, and medical personnel numbers.
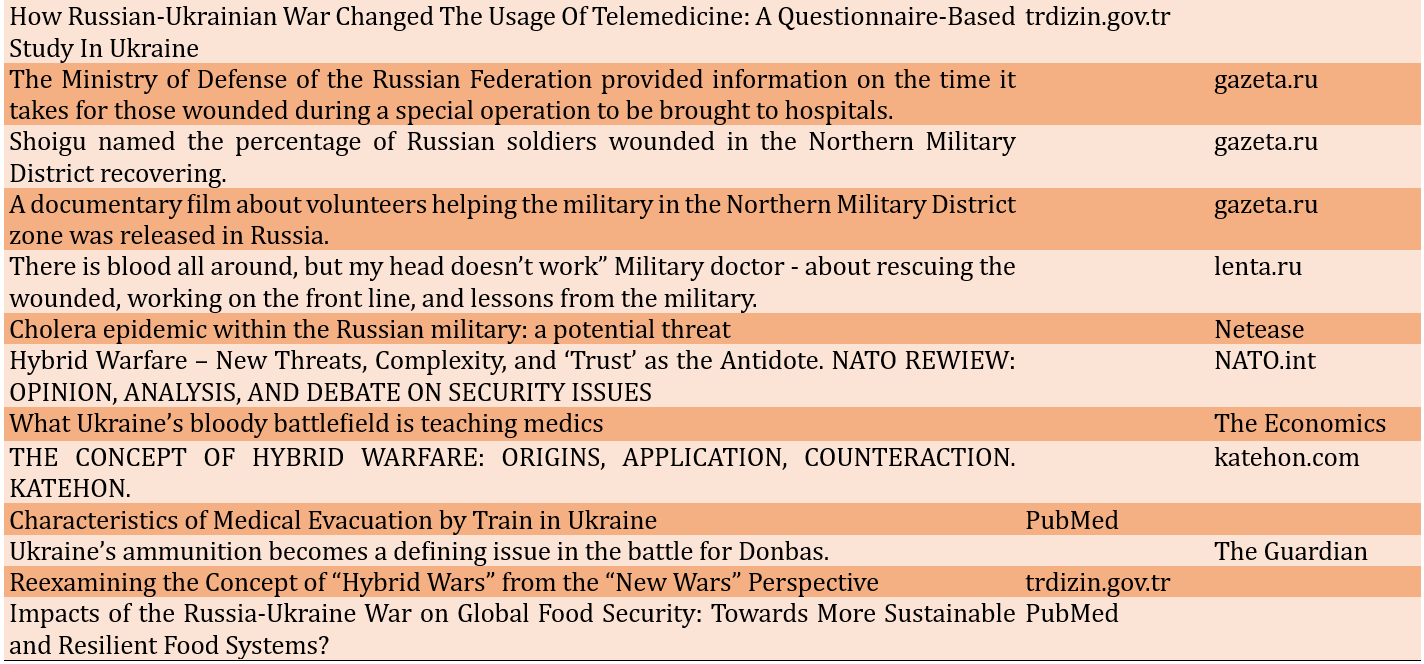
We studied 7 articles from PubMed, 3 from Elsevier, 2 from Google Scholar, and 2 from TrDizin, an international scientific directory. Additionally, we identified nine news articles from BBC, China Youth Daily, gazeta.ru, lenta.ru, katehon.com, and Netease, and 2 official articles from the Russian Army and NATO. We identified news and official articles via the Google Search Engine. We selected scientific articles among 343 articles. To obtain as unbiased information as possible, we accessed news and official articles by searching for information in the languages of countries such as Russia and China. It has come to our attention that evaluations from the perspective of Ukraine were generally common in scientific articles and news sites.

Figure 1. PRISMA Diagram of Searching
We classified obtained knowledge and problem areas as preventive, therapeutic, rehabilitative, and health-promoting services in the warfare about military healthcare for Russia and Ukraine in terms of principles of military medicine. The war was evaluated in terms of military medical services, and classified problem areas were discussed by comparison with principles of military medical services in conventional, counterterrorism, and hybrid warfare prior to the war.
Findings
By the end of 2022, in Ukraine, it had occurred 1000 attacks on the healthcare system, 399 of them on hospitals, which were 9% of Ukraine’s health facilities. Moreover, 65 ambulances and 86 medical personnel had been attacked by January 2023 [14]. Many of these hospitals had been targeted deliberately since drones were used before attacks, and attacks were applied repeatedly. Doctors were arrested, detained, and threatened, according to eyewitnesses.
International data shows that both countries lost people to war, emigration, and other conflicts. Yearly population growth rates of both sides accelerated to a negative trend in 2022 and 2023 (Figure 2). This means that, at the same time, both sides lost the chance to educate quality people in the public as medical people in a short time.
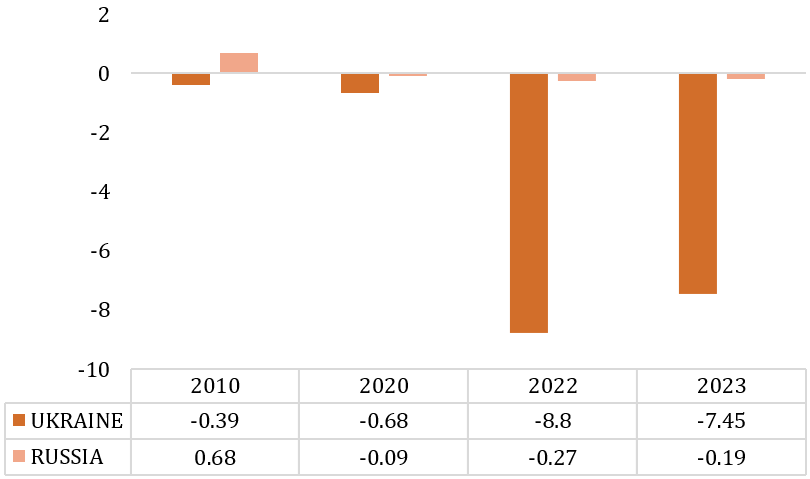
Figure 2. Yearly Population Grate Rates [15, 16]
Ukraine’s health system is undermined sharply by childhood vaccination. It’s estimated that infectious diseases such as diphtheria, measles, and polio incline in areas under the control of Russia. Chronic illnesses such as cardiovascular, mental, and renal incline due to the decline of periodic medical care to people [17].
In Ukraine, Russian forces have used modern portable antitank-guided missiles. These thermobaric weapons cause blunt and penetrating wounds as well as massive injuries [3]. These thermobaric weapons are lethal and can cause burns of the body 80% in 60 meters, which means that the weapons used in the Ukraine-Russia war are lethal at 60 meters 100%, despite evacuation in the first 72 hours. These weapons have been used in terrorist conflicts in global or local terror also, but when artillery attacks and some mortar attacks are accomplished with those kind of missiles, military medical services will need to have near, comfortable, and complete “Damage Control Surgery” and “Further Line Hospitals” for effective evacuation and treatment because of mass wounded and profound injuries.
It is claimed that Russia has been firing 60.000 artillery rounds for a day; this is equal to the volume that the US was exposed to in World War 2 for a day [18]. Artillery and rockets are responsible for 70% of injuries on the battlefield, and these injuries arise from muchly polytraumas. Ukrainian Surgeons worked on 100 wounded soldiers, and they determined that the Injury Severity Score (ISS) exceeded 36 for those wounded who were victims of barrage artillery and rocket attacks [3]. However, ISS is generally 15-25 in counterterrorism operations; for example, a study showed that of 70 Turkish Armed Forces military personnel, ISS was 21 in wounded soldiers of counterterrorism operations in 2022 [19]. Moreover, a study from 2007 to 2020 on prehospital patient activities suggested that ISS was an average of 9 in Battalion Aid Station (BAS) for injured in counterterrorism operations; the study was held with 28.950 patients, of which 3.1% (884) had prehospital visits to a BAS [20]. While the casualty rate for soldiers was 1,3-2% in Global Counterterrorism Operations of the United States, in Ukraine, this rate was estimated as 5-10% for soldiers deployed to theater operations [3].
The admission of large numbers of heavily injured soldiers is another problem for limited resources medical units on the battlefield. There were 200 wounded applied to Damage Control Surgery units for three weeks in Ukraine, according to a study from Ukrainian surgeons. They implemented laparotomy for 36 of these wounded and thoracotomy for 20 of them. These injured soldiers have taught us about body armor as well. Body armors protect vital organs on the front and back but can’t protect the body's lateral thoracic and abdominal areas against ballistic thread from lateral trajectory [3]. This issue of injury types and treatment approaches is considerable in such wars.
87 surgeons per 100.000 people in Ukraine in 2014 [17]. This rate is 47-55 in 2013-2015 for Türkiye, 144-163 in 2013-2015 for Greece, and 91,79 in 2015 for the European :union: [21]. Holding these surgeons is difficult in terms of working circumstances and economics in warfare times, and surgeon numbers have decreased since 2014 in Ukraine because of war conditions. The American College of Surgeons threw “Military Clinical Readiness Curriculum (M-Course) for Ukraine's medical workforce, who cover more than 650 general practitioners and assistant doctors. M Course was organized to train these doctors in reconstructive surgery and biological and chemical warfare, and they have made more than 300 medical operations for the wounded [3].
Wounded who arrived at further-line medical facilities had a hemorrhagic shock rate of 25%. Furthermore, 15-20 % of injured soldiers arriving at borderline medical units used to need blood transfusions in Ukraine. Surgeons of Ukraine had to go up to 500m. to further line times to times, but the big problem in getting fresh blood in further line is loud refrigerators which are activated by electricity generators; these storage refrigerators are a threat to safety in terms of vocal discipline in the battlefield. The challenge of these obstacles is an alternative to applying the “Walking Blood Bank” strategy. However, given the operational heavy, it is underlined that these solve strategies can’t be achieved [3]. Given the surgical activities, blood transfusion services are one of the most important requirements for medical care. Until 2022, though Ukraine has a mixed model of blood transfusion services as a regional-territorial principle with almost 70 blood establishments and 600 hospital blood banks, all services for blood needs have been postponed and suspended due to the war [5].
The other claim is using incendiary ammo by Russia. These munitions bring about deep burns on the whole body, unfortunately, as well as have some toxic effects due to organophosphate poisoning. These injuries require expensive, complex, and long-term care periods [3]. If soldiers were exposed to these injuries in terror territories, they could be evacuated to safe and modern facilities in the acute term, and you can implement modern treatment techniques for the injured. However, if they were exposed to these in war, the operation of evacuation and treatment may face unsafe, destroyed, and consumed medical facilities, infrastructure, energy structure, and freshwater systems.
Ukrainian Special Surgical Groups (USSG) have provided damage control surgery as close as 0.5km from active combat areas. USSG is talented at accomplishing 10 Damage Control Surgeries and holding up 15 critical patients per 48 hours without supply [3].
These rates are equal to those of a hospital's intensive care unit. The Global Surgical and Medical Support Group (GSMSG) from the United States, a nongovernment organization that provides medical care and training in conflict zones, arrived in Ukraine on March 5, 2022, after ten days of war. Team members have trained more than 20,000 Ukrainian service members. The group has also provided surgical support to more than 300 patients, some located as close as 10km from the frontline [3].
Moreover, Ukraine had already lost hospital beds from 2014 to 2017 at a rate of 5 beds per 10,000 people. And we don’t know how about hospital beds right now under the bombardment we saw in the news. On the other hand, from 2017 to 2021, Russia lost one hospital bed per 10000 people (Figure 3). We can estimate that this situation will increase in 2022-2023.

Figure 3. Number of Hospital Beds per 10000 Population [22]
In Ukraine, military medical trains have been extensively used from east to west for 60% of military casualties [23, 24]. As well as aircraft have been used for casualties, surgical teams need more capability to work in these circumstances during hundreds of kilometers and long hours. Aircraft have been used for strategic medevac to Germany and Norway; it is coordinated by the International Military Coordination Center in Koblenz, Germany. “Project Korovai” is also an initiative by the international community to support and gift medical material to Ukraine. The project includes medical materials instead of wedding gifts, which means Korovai in Ukraine [2]. Despite medevac by aircraft being the fastest evacuation form on the battlefield, the Ukrainians were exposed to the challenge of communication, which is used to inform hospitals of the reason for cutting communication with Russia [3].
The ratio of killed in action to wounded in action has been used in Ukraine, in contrast to survival in action in Afghanistan or Iraq [2]. Compared to low-intensive conflicts, war brings about greater injuries because of the use of various ammo and weapons.
While antibiotic resistance has become a big problem in Ukraine during the war, Ukraine had required prescriptions from doctors for antibiotics just before the war. Mass of wounded, complex wounds, and environmental devastating have undermined efforts against antibiotic resistance throughout Ukraine [2].
One effect of war on civilian medical services is the acceleration in the usage of telemedicine, such as SMS, email, social media apps, and remote medical devices in Ukraine [25]. However, the results of this study, which was compiled by Ukrainian scientists, are ironic given the damage to infrastructure during the war.
There are almost 140 military hospitals in Russia, but national hospitals also accept wounded from the battlefield. Some national hospitals have set up military surgery clinics in their self-structure. Russian casualties on the battlefield got a rate of 1:3 as died:wounded. It means that it was at least 3.000 died and more than three times died in the first three months of war out of the Russian Army, even if it was much more than these numbers, according to Ukraine Intelligence [26].
Even though the “Gerasimov Doctrine” was developed as an anti-hybrid war system using all state departments, the 1991 management crisis and the 2004 economic crisis affected the civilian medical system adversely. Therefore, it seems that the medical system in war circumstances can’t be supported by the national medical system in Russia nowadays. However, the Russian civilian medical department supports military personnel with the described procedures. City clinics have been divided according to front, battlefield, or battalions of soldiers and healthcare. Murmansk City Clinic is one of them [27]. This city is near the Finland border and deployed northwest, far from the battlefield.
According to the General Approach to military medicine, battalion medical teams and mobile damage control units are suitable medical units for the Russian Army in an active battlefield because of the organization system in the form of battalions attached to divisions.
In 2022, after starting up a special operation in Ukraine, the Ministry of Defense of the Russian Federation declared that complex injured soldiers are treated in 10 minutes, are evacuated to military hospitals in 1 hour, and arrive at central hospitals in 24 hours [28]. Furthermore, it was expressed that 98% of injured soldiers were recovered and discharged by the ministry [29]. However, even though 98% of injured soldiers were recovered and discharged, Russia needed to edit and publish a documentary movie for the public about healthcare voluntariness [30].
On the battlefield, every battalion has a medical platoon that provides healthcare. According to doctors from the battlefield, despite injuries by face-to-face fighting decrease, injuries by rocket attacks, artillery attacks, and mortar attacks increase in medical platoon’s treatment units. In the area, first aid is carried out by the nearest soldier, and these soldiers take the wounded to the safety area. The wounded are evacuated to the deeper region by special ambulance. This ambulance and medical personnel construct a medical platoon. When the medical platoon moves to zero point for evacuating the wounded, another ambulance moves to the waiting point. Some wounded evacuate as deep as Moscow or St. Petersburg by airway. However, medical platoon personnel were repairmen, particularly in Marriopol, almost 100%, but now they have gained experience in battlefield medicine [31].
Doctors on the battlefield consider education in first aid and tactical medicine. Stabilizing wounded during evacuation seems to be the most important challenge before hospital healthcare.
It is claimed that medical material standardization is unsuitable for battlefields and hospitals in the Russian Army. Since medical supplies, diagnostic kits, and first aid kits differ between troops and units, learning and using medical supplies is difficult [31].
Another problem on the battlefield is a classical problem for military medicine about the command control system. Military medical professionals believe that medical command and control should be managed by military medical personnel, not by warrior personnel. However, some doctors claim that the Russian Army continues this fault [31], which has undermined armies frequently throughout history.
Blood storage is another issue on the battlefield. In Russia, military hospitals such as St. Petersburg, Belgorod, etc., have accepted blood donors. However, the problem was storing blood and blood products in the first two months of the war. Eventually, hospitals solved this problem with periodic blood donation [26].
Infectious diseases have had a catastrophic effect on armies on battlefields since the ages. Allegedly, the cholera epidemic reduced the fighting potential of the Russian army in the Kherson and Crimea regions due to dehydration, diarrhea, and vomiting and spread rapidly due to contaminated water and food [32]. This news shows us that conventional and hybrid wars in our modern age include the same risks as old and ancient wars.
Discussion
The war between Ukraine and Russia has shown that the recession period of The Walker Dip” has arrived at an end for military healthcare services in Europe and the Middle East. The Walker Dip cycle refers to improving healthcare skills for battle injuries during the conflict, followed by declining skills needed to provide this care during peacetime [33]. Military medical systems of regional countries should reacquire skills in military medicine.
The most important issue in this readiness section is the discrimination between conventional war, counterterrorism operations, and hybrid war doctrines. Because some of the activities in military medicine approaches have differences in these doctrines. The most remarkable differences are related to the deployment of medical facilities and the medevac system. However, due to its complexity, hybrid war readiness makes states ready for every war doctrine [34]. It consists of regular military forces, irregular forces, special forces, economic warfare, cyber-attacks, diplomacy, information warfare propaganda, and support for local unrest. It is described as the militarization of diplomacy [35].
When we evaluate hybrid threats in terms of health services, it is considered that the lack of human, economic, and trust between the health system and the public is bilateral. This situation is harmful and destructive on both sides. In hybrid conflict environments, where all state institutions will fight synchronously, the struggle involving health services requires the integrated cooperation and coordination of the national and military health systems. Preventive medicine was not called processed health examination, vaccination, or medical intelligence. We can understand that epidemiologic studies are not carried out for headquarters since both Ukraine and Russia have lost control of health services for the battlefield.
Regarding Therapeutic Services, one of the most important problems is that safe healthcare facilities are farther from the battlefields in Russia and Ukraine. Hospitals are deployed up to 400km in Ukraine from the battlefield, and the airway is not safe as well. In Russia, evacuation by airway can cover for hours. However, Russia can evacuate the wounded in 1 hour to medical facilities near the battlefield. It’s claimed that attacking Ukraine’s Health System and Health Staff is the strategy of Russia [17]. It is not possible also to claim that Ukraine does not harm the medical system of Russia; at least, we have no evidence. However, both sides are rapidly losing medical facilities.
Another problem is miscommunication between evacuation personnel and medical facilities when preparing for the wounded. Furthermore, migrants and the civilian public who escape from conflicted areas mandatorily increase the load of medical facilities deployed in route migration. Hospitals that are already poor in terms of material and personnel are oppressed by this great load.
The other problem area is the non-standardized application of first aid personnel and materials. Russia is under an embargo on even first aid materials, and Ukraine doesn’t consider the difference between first aid and medical treatment. First aid applications prevent death or worsening of the situation, injury, and shock; in hybrid and conventional war, the war area is vast, possibly the whole country. Artillery and rocket attacks may affect up to 500-2.000km deep. Blood storage and hospitals may have to be deployed too deep from the battlefield. Therefore, communication for medical activity becomes more important for the medical system and safety; a comprehensive and fluent communication system is required for the medical department.
By safe flying routes, attacks of rockets and air fights should be prevented for MEDEVAC. Therefore, the medical system should have its own flight and air defense systems. However, for many armies, these possibilities and abilities will be limited; thus, at the smallest unit level, Damage Control Resuscitation Units (DCRU) and Damage Control Surgery Units (DCSU) should be structured and deployed on the battlefield. Hybrid war areas are deeper than in counterterrorism operations. Thus, we have to extend the time of treatment and hosting in DCU and DCEU, which is normally 36-72 hours. Furthermore, according to some studies, medical units may need to have underground facilities and tunneling tools in inventory for deployment on the battlefield [3]. A high wall and horizontal barrier system make it safe against horizontal attacks but make it vulnerable to vertical attacks.
According to news, Putin and Zelensky considered rehabilitative services in the Russia-Ukraine war. Whether fake or true news about medical services is used in war strategy for psychological and social advantage, treatment and rehabilitative services make the army determined, brave, and self-confident.
The deficiency of medical personnel is a great problem for both sides. Still, while it is not referred to in Ukraine, Russia has published an advertisement movie for voluntary medical personnel. This movie highlights that Russia needs more medical personnel to provide healthcare to war casualties. However, we must remember that Ukraine receives medical support from Western countries, specifically from governmental and nongovernmental medical corporations in the United States.
Conclusion
Medical examination and vaccination for attending to the army, medevac distances, safety of medevac routes, loss of medical facilities and medical personnel, lack of communication between medical units, load of medical facilities that are deployed in route migration mandatorily, non-standardized first aid application, and absence of medical intelligence are main problem areas regarding medical services in the Russia-Ukraine War. In peacetime, educating medical personnel is important. They should be able to work in war situations without water, facility, electricity, or medical materials. It may be the most discriminative aspect of military medicine. This education should make military medical personnel open-minded for innovation, and medical personnel should have agility and decisiveness, be outcome-focused, and be tolerated. Moreover, other military personnel need to be educated on first aid. I claim that military personnel, without exception, have to know how to apply first aid at the best level in powered armies. Protecting the force is the special expression in military wordies. It refers to preventing force loss in terms of personnel and equipment. The most effective way to prevent personnel and equipment from loss is growing and protecting military medical personnel in peacetime. A modern military medical system is a “Force Multiplier”.
Acknowledgments: None declared.
Ethics Permissions: The opinions expressed in the article are not binding on any institution or organization. This information is only the scientific thoughts reached by the authors.
Conflict of Interest: The authors declare no conflicts of interests.
Authors’ Contribution: Özmen O (First Author), Introduction Writer/Original Researcher/ Methodologist/Discussion Writer (70%); Özmen P (Second Author), Methodologist/Assistant Researcher/Statistical Analyst (30%)
Funding/Support: None declared.
Despite there being many terrorist groups and their attacks throughout the world, we have to put forward new ideas and approaches to international hybrid warfare in terms of medical delivery systems because of the comparisons and contrasts between terrorist attacks and hybrid international wars. We know that states resort to hybrid war to circumvent existing rules of law within the scope of the use of force [1]. The best and most innovative way to do this seems to be to examine the ongoing Russia-Ukraine war regarding health delivery services, in which both national armies have their own military medical structures and systems.
This article aims to show differences in terms of the medical delivery system between new hybrid national military conflicts and classic conventional war and/or terrorist conflicts and to propose new ideas and approaches in medical preparation to challenge adversaries.
However, to evaluate medical situations in warfare, you need to go and see the battlefield as an observer. However, it is impossible to stay on the battlefield as an impartial observer in wars of the modern age because of concerns about risks to the military intelligence of parties. Instead, if you want to evaluate relying on open sources, you have to regard bilateral ideas, bias, and cheating in official media, social media, and cyberspace.
In January 2022, it was observed that Ukraine’s Field Hospitals had been moved along the northern, eastern, and southeastern borders by the International Community. “Hospitals’ movement is the circumstantial evidence of about the bloody war and commander intent”, according to Napoleon (1763-1821) [2]. The claim is that hospitals were targeted by Russian forces from the borderline to the deep of the country. Zhytomyr Hospital is deployed as far west as 400km. From the borderline, it was targeted by Russia. According to the news, attacks targeted hospitals, energy, and water sources in war. Russian missiles can reach Ukraine's western, up to 20km from the Polish border. This means that the entire Ukraine is considered to be under Russian missile influence [3]. According to some reports, red cross emblems and international consensus on humanitarian treatments don’t provide protection in Ukraine. Moreover, some car parks and basements have been used as medical facilities [2]. According to paper sources, attacks targeted hospitals, electricity, and other energy sources in Ukraine and increased HIV/AIDS, Tuberculosis, and COVID-19 prevalences in cities [4]. In addition, notwithstanding continued studies on blood transfusion in Ukraine ever during the war, these activities have been undermined by aggressions of war [5] and affect the circumstances of wounded on the battlefield. Countries such as Poland, where most Ukrainian refugees initially migrated, helped Ukraine close the gaps in the health infrastructure that collapsed due to the war and shouldered the burden of health services, especially child immunizations, COVID-19 vaccines, and chronic disease treatments [6].
The war has adversely affected chronic patients and their treatments. Cancer patients are the group who are the most affected deeply. The reasons for adverse effects on chronic illnesses like cancers during the war are damage to the healthcare infrastructure and patient displacement. The war has interrupted both treatments and trials on cancer in both Russia and Ukraine [7]. Similarly, patients with rheumatological disorders and rheumatologists had to leave the city and country due to war effects [8]. Although telemedicine is considered a way for patients with chronic diseases, district access to the internet and limited medicine and drug logistic services are a great problem in war times.
President “Putin” has claimed that "The USA and NATO are rapidly deploying their secret biological laboratories close to Russian borders and preparing Ukraine for a big war." he said that “Ukraine has attacked the Russian people since 2014 starting from Donbas” [9]. Russia also blames Ukraine for crimes against humanity, just like Ukraine and its allies do.
Despite the Ministry of Defense of the Russian Federation’s official journal claims of opposition, according to “Military Industry Courier,” which is a military journal published in Russia, the military medical system on the battlefield is the restricting adverse factor for the military capacity of the Russian Army [10]. In 2018, it was claimed that thanks to developed measures, patient volume decreased among soldiers, an effective medevac system by airway, a telemedicine system, and a medical and psychological rehabilitation system for the army in Russia. Moreover, it had been claimed that in Kirov Military Medical Academy, capacity had been increased 8 times, 20.000 surgeries per year, 16.000 of them were complex and high technology surgeries, and a multidisciplined clinic had been set up for war injured in the academy, recently [11]. However, military strategists had predicted in 2018 that Bryansk, Orel, Kursk, and Belgorod Military Hospitals, part of the military healthcare system, would remain on the battlefield when war broke out on the Ukrainian border. This situation brought about extreme workload in poor war circumstances because of their deploy area. These hospitals had been deployed in the military, humanity, medical logistics, evacuation routes, and target routes for airstrikes by adversaries. Moreover, this route was capable of war fugitives and immigrants as well as civilians adversely affected by the war. These circumstances increased the workload of these military medical facilities, and they were near to targeting adversaries’ artillery and rocket attacks.
Besides the adverse effects of war on emergency healthcare and clinic systems, cyberattacks on healthcare are a problem nowadays. Although it was not brought to the agenda for the Russia-Ukraine war, it is known that there were 679 cyberattacks on healthcare services in the USA in 2021. This type of attack is a hybrid warfare component usually carried out by criminal hackers. This type of attack is a hybrid warfare component usually carried out by criminal hackers. These attacks targeted booking systems, medical technologic diagnostic systems, and patient records [12].
Food security, environmental pollution, increased violent behaviors by which damage to the social system, disruption of the education system, and freshwater security should be considered as components that threaten the healthcare system indirectly caused by the conflicts between Russia and Ukraine, like in every war [13].
Information and Methods
In this study, scientific literature was searched limited to 2017-2023 for “Trdizin”, and limited to 2022-2023 for “Google Scholar” and “Elsevier”, the last 5 years for “PubMed”, on military healthcare services during the Ukraine-Russia war. We have considered only published papers in peer-reviewed journals using main terms such as “Medical Services in Ukraine-Russia War” and ”Combat Casualty in Ukraine-Russia War”. Terms “injury, military, medicine, wounded, medevac” were used as secondary expressions for search in literature.
Table 1. List of Studied Articles
Furthermore, we have searched the military medical literature and news from China, Iran, the United Kingdom, Belarus, and the United States, considering the deception, secrecy, and the use of the media principles of war. We used the English language for all scientific literature searching, but for news, we used the Google Translate application to translate from Chinese, Persian, and Russian to English.
We confirmed all the information we obtained by comparing the official sites of governmental and nongovernmental corporations, and we highlighted some of the information we found suspicious in the article. World Health Organization database, OECD database, European :union: database, and official websites of the Ministries of Defense of both states have been used for official demographic information, including wounded and died numbers, types of casualties, and medical personnel numbers.
We studied 7 articles from PubMed, 3 from Elsevier, 2 from Google Scholar, and 2 from TrDizin, an international scientific directory. Additionally, we identified nine news articles from BBC, China Youth Daily, gazeta.ru, lenta.ru, katehon.com, and Netease, and 2 official articles from the Russian Army and NATO. We identified news and official articles via the Google Search Engine. We selected scientific articles among 343 articles. To obtain as unbiased information as possible, we accessed news and official articles by searching for information in the languages of countries such as Russia and China. It has come to our attention that evaluations from the perspective of Ukraine were generally common in scientific articles and news sites.
Figure 1. PRISMA Diagram of Searching
We classified obtained knowledge and problem areas as preventive, therapeutic, rehabilitative, and health-promoting services in the warfare about military healthcare for Russia and Ukraine in terms of principles of military medicine. The war was evaluated in terms of military medical services, and classified problem areas were discussed by comparison with principles of military medical services in conventional, counterterrorism, and hybrid warfare prior to the war.
Findings
By the end of 2022, in Ukraine, it had occurred 1000 attacks on the healthcare system, 399 of them on hospitals, which were 9% of Ukraine’s health facilities. Moreover, 65 ambulances and 86 medical personnel had been attacked by January 2023 [14]. Many of these hospitals had been targeted deliberately since drones were used before attacks, and attacks were applied repeatedly. Doctors were arrested, detained, and threatened, according to eyewitnesses.
International data shows that both countries lost people to war, emigration, and other conflicts. Yearly population growth rates of both sides accelerated to a negative trend in 2022 and 2023 (Figure 2). This means that, at the same time, both sides lost the chance to educate quality people in the public as medical people in a short time.
Figure 2. Yearly Population Grate Rates [15, 16]
Ukraine’s health system is undermined sharply by childhood vaccination. It’s estimated that infectious diseases such as diphtheria, measles, and polio incline in areas under the control of Russia. Chronic illnesses such as cardiovascular, mental, and renal incline due to the decline of periodic medical care to people [17].
In Ukraine, Russian forces have used modern portable antitank-guided missiles. These thermobaric weapons cause blunt and penetrating wounds as well as massive injuries [3]. These thermobaric weapons are lethal and can cause burns of the body 80% in 60 meters, which means that the weapons used in the Ukraine-Russia war are lethal at 60 meters 100%, despite evacuation in the first 72 hours. These weapons have been used in terrorist conflicts in global or local terror also, but when artillery attacks and some mortar attacks are accomplished with those kind of missiles, military medical services will need to have near, comfortable, and complete “Damage Control Surgery” and “Further Line Hospitals” for effective evacuation and treatment because of mass wounded and profound injuries.
It is claimed that Russia has been firing 60.000 artillery rounds for a day; this is equal to the volume that the US was exposed to in World War 2 for a day [18]. Artillery and rockets are responsible for 70% of injuries on the battlefield, and these injuries arise from muchly polytraumas. Ukrainian Surgeons worked on 100 wounded soldiers, and they determined that the Injury Severity Score (ISS) exceeded 36 for those wounded who were victims of barrage artillery and rocket attacks [3]. However, ISS is generally 15-25 in counterterrorism operations; for example, a study showed that of 70 Turkish Armed Forces military personnel, ISS was 21 in wounded soldiers of counterterrorism operations in 2022 [19]. Moreover, a study from 2007 to 2020 on prehospital patient activities suggested that ISS was an average of 9 in Battalion Aid Station (BAS) for injured in counterterrorism operations; the study was held with 28.950 patients, of which 3.1% (884) had prehospital visits to a BAS [20]. While the casualty rate for soldiers was 1,3-2% in Global Counterterrorism Operations of the United States, in Ukraine, this rate was estimated as 5-10% for soldiers deployed to theater operations [3].
The admission of large numbers of heavily injured soldiers is another problem for limited resources medical units on the battlefield. There were 200 wounded applied to Damage Control Surgery units for three weeks in Ukraine, according to a study from Ukrainian surgeons. They implemented laparotomy for 36 of these wounded and thoracotomy for 20 of them. These injured soldiers have taught us about body armor as well. Body armors protect vital organs on the front and back but can’t protect the body's lateral thoracic and abdominal areas against ballistic thread from lateral trajectory [3]. This issue of injury types and treatment approaches is considerable in such wars.
87 surgeons per 100.000 people in Ukraine in 2014 [17]. This rate is 47-55 in 2013-2015 for Türkiye, 144-163 in 2013-2015 for Greece, and 91,79 in 2015 for the European :union: [21]. Holding these surgeons is difficult in terms of working circumstances and economics in warfare times, and surgeon numbers have decreased since 2014 in Ukraine because of war conditions. The American College of Surgeons threw “Military Clinical Readiness Curriculum (M-Course) for Ukraine's medical workforce, who cover more than 650 general practitioners and assistant doctors. M Course was organized to train these doctors in reconstructive surgery and biological and chemical warfare, and they have made more than 300 medical operations for the wounded [3].
Wounded who arrived at further-line medical facilities had a hemorrhagic shock rate of 25%. Furthermore, 15-20 % of injured soldiers arriving at borderline medical units used to need blood transfusions in Ukraine. Surgeons of Ukraine had to go up to 500m. to further line times to times, but the big problem in getting fresh blood in further line is loud refrigerators which are activated by electricity generators; these storage refrigerators are a threat to safety in terms of vocal discipline in the battlefield. The challenge of these obstacles is an alternative to applying the “Walking Blood Bank” strategy. However, given the operational heavy, it is underlined that these solve strategies can’t be achieved [3]. Given the surgical activities, blood transfusion services are one of the most important requirements for medical care. Until 2022, though Ukraine has a mixed model of blood transfusion services as a regional-territorial principle with almost 70 blood establishments and 600 hospital blood banks, all services for blood needs have been postponed and suspended due to the war [5].
The other claim is using incendiary ammo by Russia. These munitions bring about deep burns on the whole body, unfortunately, as well as have some toxic effects due to organophosphate poisoning. These injuries require expensive, complex, and long-term care periods [3]. If soldiers were exposed to these injuries in terror territories, they could be evacuated to safe and modern facilities in the acute term, and you can implement modern treatment techniques for the injured. However, if they were exposed to these in war, the operation of evacuation and treatment may face unsafe, destroyed, and consumed medical facilities, infrastructure, energy structure, and freshwater systems.
Ukrainian Special Surgical Groups (USSG) have provided damage control surgery as close as 0.5km from active combat areas. USSG is talented at accomplishing 10 Damage Control Surgeries and holding up 15 critical patients per 48 hours without supply [3].
These rates are equal to those of a hospital's intensive care unit. The Global Surgical and Medical Support Group (GSMSG) from the United States, a nongovernment organization that provides medical care and training in conflict zones, arrived in Ukraine on March 5, 2022, after ten days of war. Team members have trained more than 20,000 Ukrainian service members. The group has also provided surgical support to more than 300 patients, some located as close as 10km from the frontline [3].
Moreover, Ukraine had already lost hospital beds from 2014 to 2017 at a rate of 5 beds per 10,000 people. And we don’t know how about hospital beds right now under the bombardment we saw in the news. On the other hand, from 2017 to 2021, Russia lost one hospital bed per 10000 people (Figure 3). We can estimate that this situation will increase in 2022-2023.
Figure 3. Number of Hospital Beds per 10000 Population [22]
In Ukraine, military medical trains have been extensively used from east to west for 60% of military casualties [23, 24]. As well as aircraft have been used for casualties, surgical teams need more capability to work in these circumstances during hundreds of kilometers and long hours. Aircraft have been used for strategic medevac to Germany and Norway; it is coordinated by the International Military Coordination Center in Koblenz, Germany. “Project Korovai” is also an initiative by the international community to support and gift medical material to Ukraine. The project includes medical materials instead of wedding gifts, which means Korovai in Ukraine [2]. Despite medevac by aircraft being the fastest evacuation form on the battlefield, the Ukrainians were exposed to the challenge of communication, which is used to inform hospitals of the reason for cutting communication with Russia [3].
The ratio of killed in action to wounded in action has been used in Ukraine, in contrast to survival in action in Afghanistan or Iraq [2]. Compared to low-intensive conflicts, war brings about greater injuries because of the use of various ammo and weapons.
While antibiotic resistance has become a big problem in Ukraine during the war, Ukraine had required prescriptions from doctors for antibiotics just before the war. Mass of wounded, complex wounds, and environmental devastating have undermined efforts against antibiotic resistance throughout Ukraine [2].
One effect of war on civilian medical services is the acceleration in the usage of telemedicine, such as SMS, email, social media apps, and remote medical devices in Ukraine [25]. However, the results of this study, which was compiled by Ukrainian scientists, are ironic given the damage to infrastructure during the war.
There are almost 140 military hospitals in Russia, but national hospitals also accept wounded from the battlefield. Some national hospitals have set up military surgery clinics in their self-structure. Russian casualties on the battlefield got a rate of 1:3 as died:wounded. It means that it was at least 3.000 died and more than three times died in the first three months of war out of the Russian Army, even if it was much more than these numbers, according to Ukraine Intelligence [26].
Even though the “Gerasimov Doctrine” was developed as an anti-hybrid war system using all state departments, the 1991 management crisis and the 2004 economic crisis affected the civilian medical system adversely. Therefore, it seems that the medical system in war circumstances can’t be supported by the national medical system in Russia nowadays. However, the Russian civilian medical department supports military personnel with the described procedures. City clinics have been divided according to front, battlefield, or battalions of soldiers and healthcare. Murmansk City Clinic is one of them [27]. This city is near the Finland border and deployed northwest, far from the battlefield.
According to the General Approach to military medicine, battalion medical teams and mobile damage control units are suitable medical units for the Russian Army in an active battlefield because of the organization system in the form of battalions attached to divisions.
In 2022, after starting up a special operation in Ukraine, the Ministry of Defense of the Russian Federation declared that complex injured soldiers are treated in 10 minutes, are evacuated to military hospitals in 1 hour, and arrive at central hospitals in 24 hours [28]. Furthermore, it was expressed that 98% of injured soldiers were recovered and discharged by the ministry [29]. However, even though 98% of injured soldiers were recovered and discharged, Russia needed to edit and publish a documentary movie for the public about healthcare voluntariness [30].
On the battlefield, every battalion has a medical platoon that provides healthcare. According to doctors from the battlefield, despite injuries by face-to-face fighting decrease, injuries by rocket attacks, artillery attacks, and mortar attacks increase in medical platoon’s treatment units. In the area, first aid is carried out by the nearest soldier, and these soldiers take the wounded to the safety area. The wounded are evacuated to the deeper region by special ambulance. This ambulance and medical personnel construct a medical platoon. When the medical platoon moves to zero point for evacuating the wounded, another ambulance moves to the waiting point. Some wounded evacuate as deep as Moscow or St. Petersburg by airway. However, medical platoon personnel were repairmen, particularly in Marriopol, almost 100%, but now they have gained experience in battlefield medicine [31].
Doctors on the battlefield consider education in first aid and tactical medicine. Stabilizing wounded during evacuation seems to be the most important challenge before hospital healthcare.
It is claimed that medical material standardization is unsuitable for battlefields and hospitals in the Russian Army. Since medical supplies, diagnostic kits, and first aid kits differ between troops and units, learning and using medical supplies is difficult [31].
Another problem on the battlefield is a classical problem for military medicine about the command control system. Military medical professionals believe that medical command and control should be managed by military medical personnel, not by warrior personnel. However, some doctors claim that the Russian Army continues this fault [31], which has undermined armies frequently throughout history.
Blood storage is another issue on the battlefield. In Russia, military hospitals such as St. Petersburg, Belgorod, etc., have accepted blood donors. However, the problem was storing blood and blood products in the first two months of the war. Eventually, hospitals solved this problem with periodic blood donation [26].
Infectious diseases have had a catastrophic effect on armies on battlefields since the ages. Allegedly, the cholera epidemic reduced the fighting potential of the Russian army in the Kherson and Crimea regions due to dehydration, diarrhea, and vomiting and spread rapidly due to contaminated water and food [32]. This news shows us that conventional and hybrid wars in our modern age include the same risks as old and ancient wars.
Discussion
The war between Ukraine and Russia has shown that the recession period of The Walker Dip” has arrived at an end for military healthcare services in Europe and the Middle East. The Walker Dip cycle refers to improving healthcare skills for battle injuries during the conflict, followed by declining skills needed to provide this care during peacetime [33]. Military medical systems of regional countries should reacquire skills in military medicine.
The most important issue in this readiness section is the discrimination between conventional war, counterterrorism operations, and hybrid war doctrines. Because some of the activities in military medicine approaches have differences in these doctrines. The most remarkable differences are related to the deployment of medical facilities and the medevac system. However, due to its complexity, hybrid war readiness makes states ready for every war doctrine [34]. It consists of regular military forces, irregular forces, special forces, economic warfare, cyber-attacks, diplomacy, information warfare propaganda, and support for local unrest. It is described as the militarization of diplomacy [35].
When we evaluate hybrid threats in terms of health services, it is considered that the lack of human, economic, and trust between the health system and the public is bilateral. This situation is harmful and destructive on both sides. In hybrid conflict environments, where all state institutions will fight synchronously, the struggle involving health services requires the integrated cooperation and coordination of the national and military health systems. Preventive medicine was not called processed health examination, vaccination, or medical intelligence. We can understand that epidemiologic studies are not carried out for headquarters since both Ukraine and Russia have lost control of health services for the battlefield.
Regarding Therapeutic Services, one of the most important problems is that safe healthcare facilities are farther from the battlefields in Russia and Ukraine. Hospitals are deployed up to 400km in Ukraine from the battlefield, and the airway is not safe as well. In Russia, evacuation by airway can cover for hours. However, Russia can evacuate the wounded in 1 hour to medical facilities near the battlefield. It’s claimed that attacking Ukraine’s Health System and Health Staff is the strategy of Russia [17]. It is not possible also to claim that Ukraine does not harm the medical system of Russia; at least, we have no evidence. However, both sides are rapidly losing medical facilities.
Another problem is miscommunication between evacuation personnel and medical facilities when preparing for the wounded. Furthermore, migrants and the civilian public who escape from conflicted areas mandatorily increase the load of medical facilities deployed in route migration. Hospitals that are already poor in terms of material and personnel are oppressed by this great load.
The other problem area is the non-standardized application of first aid personnel and materials. Russia is under an embargo on even first aid materials, and Ukraine doesn’t consider the difference between first aid and medical treatment. First aid applications prevent death or worsening of the situation, injury, and shock; in hybrid and conventional war, the war area is vast, possibly the whole country. Artillery and rocket attacks may affect up to 500-2.000km deep. Blood storage and hospitals may have to be deployed too deep from the battlefield. Therefore, communication for medical activity becomes more important for the medical system and safety; a comprehensive and fluent communication system is required for the medical department.
By safe flying routes, attacks of rockets and air fights should be prevented for MEDEVAC. Therefore, the medical system should have its own flight and air defense systems. However, for many armies, these possibilities and abilities will be limited; thus, at the smallest unit level, Damage Control Resuscitation Units (DCRU) and Damage Control Surgery Units (DCSU) should be structured and deployed on the battlefield. Hybrid war areas are deeper than in counterterrorism operations. Thus, we have to extend the time of treatment and hosting in DCU and DCEU, which is normally 36-72 hours. Furthermore, according to some studies, medical units may need to have underground facilities and tunneling tools in inventory for deployment on the battlefield [3]. A high wall and horizontal barrier system make it safe against horizontal attacks but make it vulnerable to vertical attacks.
According to news, Putin and Zelensky considered rehabilitative services in the Russia-Ukraine war. Whether fake or true news about medical services is used in war strategy for psychological and social advantage, treatment and rehabilitative services make the army determined, brave, and self-confident.
The deficiency of medical personnel is a great problem for both sides. Still, while it is not referred to in Ukraine, Russia has published an advertisement movie for voluntary medical personnel. This movie highlights that Russia needs more medical personnel to provide healthcare to war casualties. However, we must remember that Ukraine receives medical support from Western countries, specifically from governmental and nongovernmental medical corporations in the United States.
Conclusion
Medical examination and vaccination for attending to the army, medevac distances, safety of medevac routes, loss of medical facilities and medical personnel, lack of communication between medical units, load of medical facilities that are deployed in route migration mandatorily, non-standardized first aid application, and absence of medical intelligence are main problem areas regarding medical services in the Russia-Ukraine War. In peacetime, educating medical personnel is important. They should be able to work in war situations without water, facility, electricity, or medical materials. It may be the most discriminative aspect of military medicine. This education should make military medical personnel open-minded for innovation, and medical personnel should have agility and decisiveness, be outcome-focused, and be tolerated. Moreover, other military personnel need to be educated on first aid. I claim that military personnel, without exception, have to know how to apply first aid at the best level in powered armies. Protecting the force is the special expression in military wordies. It refers to preventing force loss in terms of personnel and equipment. The most effective way to prevent personnel and equipment from loss is growing and protecting military medical personnel in peacetime. A modern military medical system is a “Force Multiplier”.
Acknowledgments: None declared.
Ethics Permissions: The opinions expressed in the article are not binding on any institution or organization. This information is only the scientific thoughts reached by the authors.
Conflict of Interest: The authors declare no conflicts of interests.
Authors’ Contribution: Özmen O (First Author), Introduction Writer/Original Researcher/ Methodologist/Discussion Writer (70%); Özmen P (Second Author), Methodologist/Assistant Researcher/Statistical Analyst (30%)
Funding/Support: None declared.
Keywords:
References
1. Işıkçı, E, Kiraz E. Reexamining the concept of "Hybrid Wars" from the "New Wars" Perspective. J Defence War Stud 2021;30(2):253-66. [Link]
2. Hodgetts TJ, Naumann DN, Bowley DM. Transferable military medical lessons from the Russo-Ukraine war. BMJ Mil Health. 2023:e002435. [Link] [DOI:10.1136/military-2023-002435]
3. Epstein A, Johannigman J, Fox CJ, Inaba K, Vercruysse GA. Putting medical boots on the ground: Lessons from the war in Ukraine and applications for future conflict with near-peer adversaries. J Am Coll Surg. 2023;237(2):364-373. [Link] [DOI:10.1097/XCS.0000000000000707]
4. Haque U, Naeem A, Wang S, Espinoza J, Holovanova I, Gutor I. The human toll and humanitarian crisis of the Russia-Ukraine war: the first 162 days. BMJ Glob Health. 2022;7(9):e009550. [Link] [DOI:10.1136/bmjgh-2022-009550]
5. Babynets A, Dmytruk S. The blood transfusion service of Ukraine. Transfus Apher Sci. 2023;62(5):103804. [Link] [DOI:10.1016/j.transci.2023.103804]
6. Fatyga E, Dzięgielewska-Gęsiak S, Muc-Wierzgoń M. Organization of Medical Assistance in Poland for Ukrainian Citizens During the Russia-Ukraine War. Front Public Health. 2022;10:904588. [Link] [DOI:10.3389/fpubh.2022.904588]
7. Talbot A, Connor SG, Austin K, Hannon T, Gabbay E, Clay TD. The impact of the 2022 Ukraine/Russian conflict on cancer clinical trials. J Int Med Res. 2022;50(12):03000605221143284. [Link] [DOI:10.1177/03000605221143284]
8. Doskaliuk B. How the Russian invasion affects Ukrainian rheumatological health care. Nat Rev Rheumatol. 2022;18(9):491-2. [Link] [DOI:10.1038/s41584-022-00809-0]
9. Kremlin. President of Russia (Address of the President to the Federal Assembly) [Internet]. Moscow: Kremlin.ru; 2023 Feb -[2023 May 21]. Available from: http://kremlin.ru/events/president/news/70565. [Russian] [Link]
10. Cyol. Russian military medical system sounds alarm [Internet]. Beijing:Cyol; 2018 Feb- 2023 June 11]. Available from: http://qnck.cyol.com/html/2018-02/28/nw.D110000qnck_20180228_2-06.htm. [Chinese] [Link]
11. Tikhonov A. Ambitious tasks should always be set for yourself [Internet]. Moscow: Army Collection; 2018 Dec-[2023 June 11]. Available from: https://army.ric.mil.ru/Stati/item/156804/. [Russian] [Link]
12. Granholm F, Tin D, Ciottone GR. Not war, not terrorism, the impact of hybrid warfare on emergency medicine. Am J Emerg Med. 2022;62:96-100. [Link] [DOI:10.1016/j.ajem.2022.10.021]
13. Hassen TB, El Bilali H. Impacts of the Russia-Ukraine War on Global Food Security: Towards More Sustainable and Resilient Food Systems?. Foods. 2022;11(15):2301. [Link] [DOI:10.3390/foods11152301]
14. Mahase E. Ukraine: Over 700 recorded attacks on health facilities and workers in year since Russia invasion. BMJ. 2023;380. [Link] [DOI:10.1136/bmj.p451]
15. Wordometer (Ukraine). Ukraine Population (LIVE) Yearly Population Growth Rate (%) [Internet]. Chicago: Wordometer; [2023 September 10]. Available from: https://www.worldometers.info/world-population/ukraine-population/. [Link]
16. Worldometer (Russia). Russia Population (LIVE) Yearly Population Growth Rate (%). [Internet]. Chicago: Wordometer; [2023 September 10]. Available from: https://www.worldometers.info/world-population/russia-population/. [Link]
17. Lancet T. Russia's invasion of Ukraine: an attack on health. Lancet. 2023;401(10377):617. [Link] [DOI:10.1016/S0140-6736(23)00387-2]
18. Beaumont P. Ukraine's ammunition becomes defining issue in battle for Donbas [Internet]. London: The Guardian.; 2022. [Cited 2023 Sep 9]. Available from: https://www.theguardian.com/world/2022/jun/27/ukraine-ammunition-becomes-defining-issue-in-battle-for-donbas. [Link]
19. Öztürk A, Şenocak R, Kaymak S, Hançerlioğulları O, Utku Çelik S, Zeybek N. Injury mechanisms and injury severity scores as determinants of urban terrorism-related thoracoabdominal injuries. Turk J Surg. 2022;38(1):67-73. [Link] [DOI:10.47717/turkjsurg.2022.5506]
20. Fisher AD, April MD, Naylor JF, Kotwal RS, Schauer SG. The battalion aid station-the forgotten frontier of the army health system during the global war on terrorism. Mil Med. 2023;188(5-6):e1240-5. [Link] [DOI:10.1093/milmed/usab401]
21. Roser M. Specialist surgical workforce (per 100,000 population) [Internet]. London: Our World In DATA. [2023 April 10]. Available from: https://ourworldindata.org/grapher/surgeons-per-100000?tab=table. [Link]
22. Statista (Ukraine and Russia). Number of hospital beds per 10,000 population in Russia from 2008 to 2021 and Number of hospital beds per 10,000 population in Ukraine from 2008 to 2017 [Internet]. New York: Statista. [2023 August 10]. Available from: https://www.statista.com/statistics/892554/density-of-hospital-beds-in-ukraine/ [Link]
23. Walravens S, Zharkova A, De Weggheleire A, Burton M, Cabrol J-C, Lee JS. Characteristics of Medical Evacuation by Train in Ukraine, 2022. JAMA Netw Open. 2023;6(6):e2319726. [Link] [DOI:10.1001/jamanetworkopen.2023.19726]
24. What Ukraine's bloody battlefield is teaching medics [Internet]. New York: The Economist. [Cited 2023 Sep 16]. Available from: https://www.economist.com/international/2023/08/04/what-ukraines-bloody-battlefield-is-teaching-medics. [Link]
25. Poberezhets V, Demchuk A, Mostovoy Y. How Russian-Ukrainian war changed the usage of telemedicine: A questionnaire-based study in Ukraine. Ankara Med J. 2022;22(3):305-18 [Link] [DOI:10.5505/amj.2022.08455]
26. BBC News. Cargo 300. Where are Russian soldiers wounded in the war in Ukraine evacuated and how are they treated? [Internet]. London: BBC News. 2022-[2023 July 10]. Available from: https://www.bbc.com/russian/features-61628388. [Link]
27. State regional budgetary healthcare institution "Murmansk City Clinic No. 2". A separate category of citizens. Murmansk: State Budgetary Institution; 2022- [2023 July 10]. Available from: https://mgpol2.ru/главная-страница-для-пациентов/порядок-оказания-медицинской-помощи/. [Russian] [Link]
28. Demidov A. The Ministry of Defense of the Russian Federation told how long it takes for those wounded during a special operation to be brought to hospitals [Internet]. Moscow:Gazeta.Ru; 2022 Nov-[2023 July 28]. Available from: https://www.gazeta.ru/army/news/2022/12/19/19302163.shtml?updated. [Russian] [Link]
29. Dmitrova D. Shoigu named the percentage of Russian soldiers wounded in the Northern Military District recovering. Moscow: Gazeta.Ru. 2022 Oct-[2023 October 3]. Available from: https://www.gazeta.ru/army/news/2023/10/03/21416845.shtml. [Russian] [Link]
30. Stolts Y. A documentary film about volunteers helping the military in the Northern Military District zone was released in Russia. Moscow: Gazeta.Ru; 2023 Sep-[2023 October 15]. Available from: https://www.gazeta.ru/culture/news/2023/09/28/21382267.shtml. [Russian] [Link]
31. Kirillov M. "There is blood all around, but my head doesn't work" Military doctor-about rescuing the wounded, working on the front line and lessons from the military military [Internet]. Moscow: Lenta.Ru. 2023 Nov-[2023 May 11]. Available from: https://lenta.ru/articles/2023/05/11/zeberg/.[Russian] [Link]
32. Zhiqiang Z. Cholera epidemic within the Russian military: a potential threat [Internet]. Binjiang:NetEase. 2023 Jul-[2023 June 21]. Available from: https://www.163.com/dy/article/I7OTNH8L05561WO8.html. [Chinese] [Link]
33. Jensen G, Egmond T, Örtenwall P, Peralta R, Aboutanos MB, Galante J. Military civilian partnerships: International proposals for bridging the Walker Dip. J Trauma Acute Care Surg. 2020;89(2S Suppl 2):S4-7. [Link] [DOI:10.1097/TA.0000000000002785]
34. Arsalan B. Hybrid warfare-new threats, complexity, and 'trust' as the antidote [Internet]. Lisbon: NATO Rewiew; 2021 Nov-[2023 September 30]. Available from: https://www.nato.int/docu/review/articles/2021/11/30/hybrid-warfare-new-threats-complexity-and-trust-as-the-antidote/index.html. [Link]
35. Savin L. The concept of hybrid warfare: Origins, application, counteraction [Internet]. Moscow: Katehon. 2021 Nov-[2023 September 21]. Available from: https://katehon.com/en/article/concept-hybrid-warfare-origins-application-counteraction. [Link]