
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

1.0
Cite Score 2025
SJR: 0.129 / SNIP: 0.140
Volume 15, Issue 1 (2023)
Iran J War Public Health 2023, 15(1): 93-99 |
Back to browse issues page
Article Type:
Subject:







History
Received: 2022/08/28 | Accepted: 2023/03/14 | Published: 2023/04/12
Received: 2022/08/28 | Accepted: 2023/03/14 | Published: 2023/04/12
How to cite this article
Nobakht R, Rostamalizadeh V, Kiani R. Quality of Life and Health of Rural Elderly; Determinants and Policy Requirements. Iran J War Public Health 2023; 15 (1) :93-99
URL: http://ijwph.ir/article-1-1227-en.html
URL: http://ijwph.ir/article-1-1227-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:


1- Department of Social Science, Payam Noor University, Tehran, Iran
2- Department of Migration and Urbanization, National Institute for Population Research (NIPR), Tehran, Iran
3- Department of Population and Health, National Population Research Institute (NIPR), Tehran, Iran
2- Department of Migration and Urbanization, National Institute for Population Research (NIPR), Tehran, Iran
3- Department of Population and Health, National Population Research Institute (NIPR), Tehran, Iran
Full-Text (HTML) (1196 Views)
Introduction
One of the long-term consequences of increasing life expectancy and changing the age structure is the aging of the population. Population aging is inevitable for countries that have experienced mortality reduction and health and social development [1]. As a developing society, Iran is also facing this phenomenon. The increase in the elderly population is different from the growth of the population of other age groups, and recent evidence based on the 2016 census shows that the rate of growth has increased [2]. The elderly population of Iran aged 60 and above will increase from a little over 7.4 million people in 2016 to nearly 33.4 million people in 2056 [3]. In other words, until that year, more than a quarter of the country's population is made up of elderly people.
In the rural society of Iran, although life expectancy in villages is lower than in cities [4], due to high migration from rural to urban areas, especially rural youth migration, the proportion of the elderly population in rural areas is higher than in urban areas [5, 6]. For example, in 2011, based on the relative distribution of the population in terms of major age groups, 6.5% in rural areas and 5.4% in urban areas were in the age groups above 65 years, which shows the difference in the proportion of the elderly population in cities and villages [7].
Elderly issues are recognized as a research priority in developed countries to determine the psychological, social, and health needs of the elderly. But despite little attention in developing countries, there is a great need for research on various aspects of elderly people in these countries. Because the issue of old age, especially for the poor elderly in third-world countries, where welfare systems are less extensive, is a very important action [8].
In these countries, especially in Iran, people in society need formal and informal support from the government, social institutions, and people around them to achieve a better quality of life and solve their problems, especially in old age [9]. In traditional societies, social support during old age was provided by children, relatives, neighborhood members, and religious networks, respectively. Now, over time, the change in the function of the family in today's societies, the evolution of the family system from extended to the nuclear family, women's employment, etc. has led to a change in support patterns, and a part of the support that was provided by family and relatives in the past has now been transferred to official and defined institutions, such as government health care and private retirement organizations [10]. Therefore, considering the changes made in the Iranian society, especially the rural society, and also considering that most of the villagers are less covered by insurance due to the characteristics of the labor market in rural areas [6], the quality of life of the rural elderly has been affected [11], and in general the quality of life in villages is often lower [12].
The World Health Organization (WHO) defines quality of life as people's perception of their position in life based on the value systems and culture in which they live and in relation to their goals, expectations, standards, and concerns [8]. Also, in another definition, quality of life is defined as a concept with several domains, including mental and physical health, social functioning, and emotional/emotional well-being [13]. In general, it can be said that the quality of life is a multi-dimensional construct, consisting of the objective conditions of life and mental well-being [14, 15]. The objective dimension includes the apparent and tangible state of life, and the subjective dimension includes people's perceptions and values of their life situation [16]. It should be acknowledged that the quality of life and the possibility of a better life are strongly affected by time and place, and its components and factors change according to the time period and geographical location [14, 16].
Also, it seems that the elderly who live in the villages are at risk of reducing their quality of life compared to their counterparts in the cities due to the specific economic and social factors of the rural environment. These factors include geographic and social separation from the larger urban community, limited access to specialized care, and possibly lower socio-economic status [17]. Surveys also show that there are differences between urban and rural communities in access to quality of life indicators, and the quality of life of rural communities is in unfavorable conditions compared to urban residents [18].
Considering that Iran is one of the countries that has a large young population that will form the elderly population in the future [19], and as mentioned, the proportion of elderly people in villages is more than in cities, so it is necessary to pay attention to their quality of life. If proper planning is not implemented to take care of the physical, mental and social health of the elderly in rural areas, the society will face many problems in this field in the future [6]. Investigating the quality of life of rural elderly can be useful for recognizing, monitoring and evaluating previous policy strategies, designing future policies and plans, as well as identifying human priorities in life, causes of people's dissatisfaction, etc. [18]. In addition, most of the studies on the quality of life in Iran have been conducted in terms of location in urban areas and fewer have been addressed in rural areas [20], and in the case of rural elderly, it has been much less.
The review of the literature shows that to determine and measure the quality of life of the elderly in rural areas, it is necessary to pay attention to both subjective and objective dimensions, and three important dimensions, namely physical health, social and environmental functions, and emotional and mental well-being in the works of researchers such as Yazdanpour and Saam Aram [21], Baernholdt et al. [13], Alizadeh et al. [16] and Dongre and Deshmukh [22] have been considered.
Regarding the factors that determine the quality of life of the elderly in rural areas, the studies of Yazdanpour and Saam Aram [21], Hajihashemi et al. [17], Farhadi et al. [23], Rezvani et al. [24], Joshi et al. Dongre and Deshmukh [22], Banjare et al. [25] and Baernholdt et al. [13] have examined demographic variables as well as social and economic variables such as housing ownership status, level of communication with family members, support, participation, spiritual status, feeling of loneliness, income status, and such things.
This research aimed to investigate the quality of life of the rural elderly in the southern counties of Fars province (Lamard and Mehr counties) and the determining factors affecting it.
Instruments and Methods
The present research is a survey study. The research population was the elderly of Lamard and Mehr cities in the south of Fars province (12151 people aged 60 and above) in 2021. Based on Cochran's formula, the sample size for each city was calculated as 372 people. However, due to the geographical distribution of the region and the importance of the subject under study, the sample was increased to 825 people. Then, with the cluster sampling method, the target area was divided into 18 main blocks based on the number of rural districts. In the second stage, 4 blocks were selected from Lamard City and 3 blocks from Mehr City. Then, a number of villages were selected from the rural district (block) and finally, in a systematic way (based on the list of the health network of the rural district center of the population over 60 years old for each village), the target sample was selected, and data was collected.
The tool for collecting data in the survey is questionnaire. In addition to the demographic questions, the main part of the questionnaire was related to the measurement of the concepts of different aspects of the quality of life as well as its determinants. The World Health Organization Quality of Life (WHOQOL) was used to assess the dimensions of quality of life based on mental-psychological status, physical health, and social- environmental status. The concept of loneliness was measured according to the study of Zarghami and Mahmoudian [26]. In Zarghami and Mahmoudian's study, the feeling of loneliness was evaluated according to UCLA's modified loneliness scale, which includes 20 items, and its shorter 3-item form, as well as De Jong Gierveld Scale, which includes 11 items [26].
In addition to the descriptive statistics used to present a picture of the studied sample, to check the effect of different variables, and also the most important variable explaining the concept of quality of life, the step-by-step regression method was used.
Findings
Out of 825 people in the statistical sample, 43.3% were men, and 56.7% were women. The highest percentage of respondents was in the age group of 75 years and above, with 27.6% (227 people), followed by the age groups of 60-64, 65-69, and 70-74. About 19% (151 people) of the households were single-person households. Also, about 50% (397 people) of the families had more than 3 members.
In terms of marital status, approximately 32% (264 people) were without a spouse (death or divorce), and 67% (552 people) had a spouse and were living with their spouse. Only 1.5% (12 people) of the sample did not have children, and other elderly people had at least one child. Also, most of the elderly were illiterate (62%, 208 people), and the rest (32%, 107 people) had only literacy and elementary education.
Almost 80% stated that their living expenses are less than 1.5 million Tomans, and it seems that since about 90% (715 people) had housing, the lack of housing costs has a role in the low costs. Children and spouse (according to income from inherited land and household work) were the most important financial supporters.
20% (165 people) of the elderly expressed their feeling of loneliness much and very much. Also, 76% (627 people) of elderly people were satisfied with their health status.
Based on the physical health aspect, about 18% (148 people) of the elderly reported low quality of life, 37% average (305 people) and 45% (372 people) high. The mental-psychological dimension of quality of life was almost the same as the physical health dimension. Based on the social- environmental dimension, 35% (289 people) of people rated their quality of life low, and almost 48% (396 people) rated it high.
Physical dimension
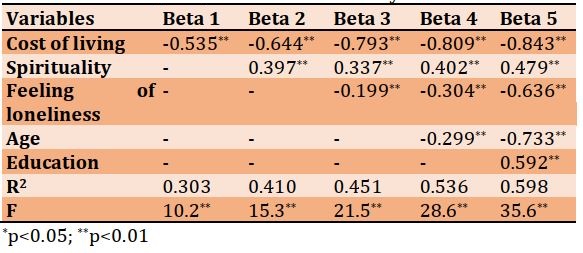
The effect of the total independent variables of gender, age, number of family members, marital status, number of children, education, cost of living, housing condition, spirituality, feeling of loneliness, and the type of financial aid on the physical dimension of the quality of life of the elderly was investigated using the step-by-step regression method. In the first step, the cost of living variable was entered into the model as the most important variable. The coefficient of determination (R2) calculated from the first model showed that the cost of living explains 30% of the changes in the quality of life (physical dimension) as a dependent variable. Also, F=10.2 (p<0.01) showed that the independent variable (living expenses) entered in the first model is able to explain well the amount of changes and variance of the dependent variable. The beta regression coefficient and the t value, which determines the relative contribution of each independent variable and the significance of the effect in explaining changes in the dependent variable, indicated that the cost of living has the greatest role in predicting the dependent variable (Beta=-0.535). Therefore, the high cost of living has a negative effect on the quality of life of the elderly. In the second step, the spirituality variable had a positive effect on the quality of life of the elderly. By entering this variable, the coefficient of determination increased to 40%. In the next steps, feelings of loneliness, age, and education were entered into the model, and according to the fifth step, almost 60% of the changes in the dependent variable were explained. The variables of loneliness and age showed that the elderly who experience more loneliness and are older have a lower quality of life. The beta coefficients indicated that the cost of living and age variables have the greatest effect on the dependent variable. So, in general, the increase in living costs, age, and feeling of loneliness decrease the quality of life in the physical dimension, and education and spirituality increase it (Table 1).
Table 1) The effect of independent variables on the physical dimension of the quality of life of rural elderly in southern Fars
Mental-psychological dimension
The cost of living variable was entered as the first variable and explained 40% of the changes in the mental-psychological dimension of the quality of life. The beta regression coefficient and t value showed that living costs play the biggest role in predicting the dependent variable (Beta=-0.432). In the next steps, spirituality, feeling of loneliness, age, and education were entered into the model. The increase in living costs, feeling of loneliness, and age reduced the mental and psychological quality of life of the elderly, and spirituality and education had a positive effect on it. According to the fifth step, almost 60% of the dependent variable changes were explained. Beta coefficients indicated that the variables of living costs and age have the greatest effect on the dependent variable. In this way, the elderly, who have a higher cost of living and are at an older age, have a low quality of life in mental-psychological dimension (Table 2).
Social- environmental dimension
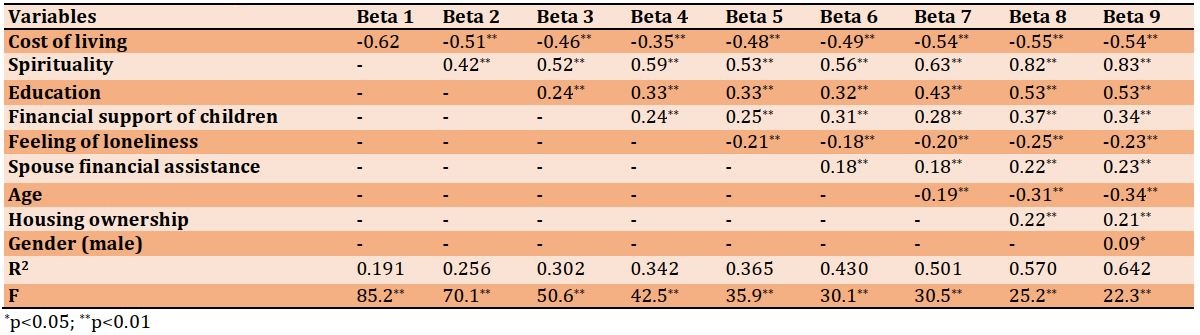
Variables were entered into the model in 9 steps. In the first step, the cost of living variable was entered into the model as the most important variable and had a negative effect on the social-environmental dimension of the quality of life of the elderly. The coefficient of determination of the first model showed that the cost of living explains 19% of the changes in the social-environmental dimension of the quality of life. In the next steps, spirituality, education, children's financial support, feelings of loneliness, spouse's financial support, age and housing ownership, and gender were entered into the model, respectively, and based on the ninth step, almost 64% of the changes in the dependent variable were explained. The beta coefficients indicated that the variable of spirituality has the highest effect, so that people who have higher spirituality also have a higher quality of life. Also, people who have a higher cost of living and feelings of loneliness and older have a lower quality of life. The financial support of children and spouses and the housing ownership also had a positive and significant effect on the social-environmental quality of life of the elderly. In this way, with the increase in living costs and feelings of loneliness, the quality of life in the social-environmental dimension decreases, and with the increase in spirituality, education, financial support, and the type of housing ownership, the quality of life of the elderly increases in the social-environmental dimension (Table 3).
Table 2) The effect of independent variables on the mentalpsychological dimension of the quality of life of rural elderly in southern Fars
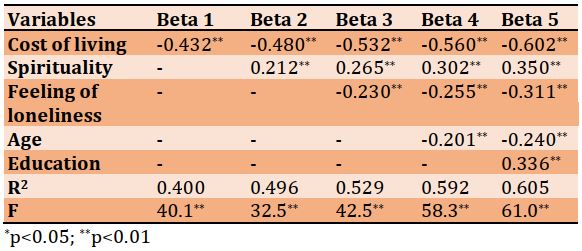
Table 3) The effect of independent variables on the social-environmental dimension of the quality of life of rural elderly in southern Fars
Quality of life in general
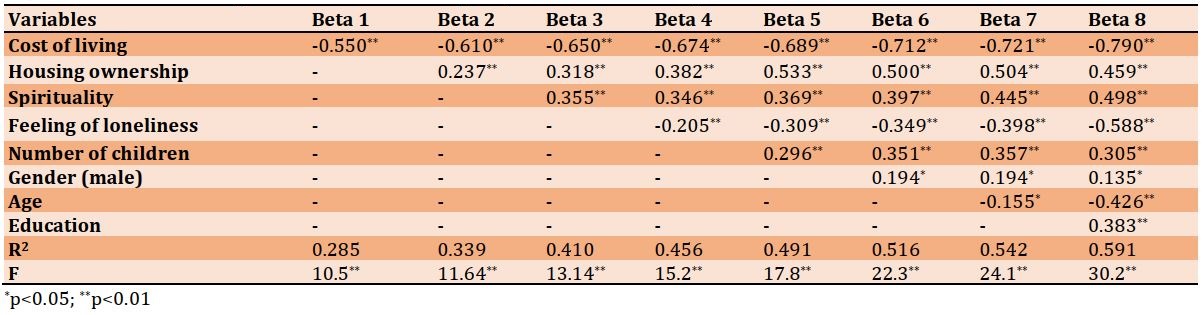
Cost of living, housing ownership, spirituality, feeling of loneliness, number of children, gender, age, and education were entered into the model as influencing variables in 8 steps. The calculated R2 indicated that in the first step, the cost of living variable explained 28% of the changes in the dependent variable, and in the final step, all variables explained 59% of the changes in the dependent variable. In all steps, the F value showed the ability of independent variables in estimating the amount of changes and variance of the dependent variable. In step 8, cost of living, feelings of loneliness, and spirituality had the highest effect. The rising cost of living, age, and feelings of loneliness had a negative effect on the quality of life of the elderly, and housing ownership, high spirituality, having children, education, and being a man had a positive effect on the quality of life (Table 4).
Table 4) The effect of independent variables on the quality of life of rural elderly in southern Fars
Discussion
Research in the field of health and the welfare of the elderly is one of the fundamental issues in public health. Today, the elderly are becoming a significant part of the country's rural population, and this trend will continue to increase in the future. Therefore, it is necessary to identify their various needs, such as psychological, social, economic, and health needs, especially at the community level, to have the necessary planning and predictions for the future. By formulating and designing appropriate and practical policies and programs, the quality of life of the elderly and their satisfaction can be improved, and the problems that may arise in this field for different sectors, such as the health system, social system, economic system, etc., can be prevented. In this regard, examining the quality of life of the rural elderly determines their current life situation and helps to identify the determining factors to improve the effective factors and design better programs. With this perspective, in this research, the quality of life of the rural elderly and its determining factors were examined.
The results of this research showed that children and spouses were the most important financial supporters of the rural elderly. Also, about 80% of the elderly felt a little lonely, which shows that living in the village and communicating more with neighbors and relatives, as well as the continuous communication of children with their parents in rural environments, has an effect on the low level of this issue. In fact, family relationships and family support during old age play an effective role in improving the quality of life of the elderly.
One of the important goals of this research was to measure the quality of life of the rural elderly. About 45% of the elderly evaluated the quality of life in physical health and mental-psychological status as high. In the social-environmental dimension, about 48% had a high quality of life.
The results show that the elderly, who have high living expenses, experience more loneliness, and are older, have a lower quality of life in terms of physical and mental health. Also, education and spirituality have a positive effect on the quality of life of the elderly in these two dimensions, which is consistent with the study of Esmaeili and Esmaeili [27] and Jadidi et al. [28]. In the social-environmental dimension, the increase in living expenses and the feeling of loneliness decrease the quality of life, which is in line with the results of Zarghami and Mahmoudian's study [26], but spirituality, education, financial support of children and spouse's financial assistance, and the type of housing increase the quality of life of the elderly in this dimension.
In general, rising cost of living, age, and feeling of loneliness have a negative effect on the health and quality of life of the rural elderly, and housing, spirituality, financial support from children, education, and being a man have a positive effect on their health and quality of life.
Regarding the negative influencing factors on the quality of life of the elderly, the findings of this research about the cost of living in the works of Yazdanpour and Saam Aram [21] and Hajihashemi et al. [17], age in the works of Joshi et al. [8] and Hajihashemi et al. [17] and the feeling of loneliness in the works of Dongre and Deshmukh [22] and Baernholdt et al. [13] have been confirmed. Here it can be said that the two important variables of living costs and feeling of loneliness are the main findings of this work, and to change and improve the quality of life of the rural elderly, attention and policies in these two variables are necessary.
Regarding the cost of living, considering that the coverage of social security insurance and social welfare in the villages is low due to the working conditions of the villagers, it is necessary to pay more attention to the rural elderly, especially in the field of their health, and diagnostic-therapeutic and welfare services and facilities should be considered for them at lower or free rates, which means there is a need for an efficient support system. Regarding the feeling of loneliness, rural elderly may be socially isolated, and therefore, they need interventions to preserve physical and mental health and strengthen social relationships and support and increase participation in society.
Another issue that was investigated in this study was the positive influencing factors on the quality of life of the elderly. In line with the results of this study, the spirituality variable has been confirmed in the study of Dongre and Deshmukh [22], the financial support of children in the study of Yazdanpour and Saam Aram [21] and the ownership of housing in the study of Joshi et al. [8]. Considering the differences between urban and rural elderly in terms of education, income, access to health facilities [23], insurance coverage, etc., rural elderly are at lower levels of quality of life. Therefore, the economic dimensions and support of children are important in order to overcome these limitations and show the perspectives of intervention and design of suitable and practical policies and programs.
This study had some limitations because it was conducted among the elderly and in a rural community. It is difficult to obtain information and research data from elderly people, and people of this age are less willing to give information. In addition, elderly people's understanding of the subjects changes with every little issue that happens to them, which makes it more difficult to investigate the research topic. For example, if an elderly person faces foot pain or other problems the day before, this will quickly affect his/her other perceptions on various issues. Another point was the statistical population of elderly rural people, who were mostly illiterate or poorly educated, and the interviewer had to speak their local language and accent, which made the data collection process very long.
It is suggested to use qualitative methods and mixed methods to know the quality of life of the rural elderly. Also, for future research, a comparison can be made between the quality of life of rural and urban elderly.
According to the results of the present study, it is necessary to pay attention to the two factors of loneliness and living expenses of the rural elderly. It is also necessary to encourage and value the support of children from elderly parents and to think of ways to continue this relationship. Regarding the access of the elderly to housing in the villages, programs should also be planned.
Conclusion
Feeling of loneliness and cost of living are two important factors in reducing the quality of life and health of rural elderly. Also, the financial support of children and the acquisition of housing plays an important role in increasing the quality of life of the rural elderly.
Acknowledgements: The authors would like to acknowledge all the people who have collaborated in the preparation of data for this article.
Ethical Permission: The questionnaire used in this research has been approved by the scientific committee of Payam Noor University, Lamard Center.
Conflict of Interests: There is no conflict of interests.
Authors’ Contribution: Nobakht R (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer (50%); Rostamalizadeh V (Second Author), Methodologist/Assistant Researcher/Discussion Writer (30%); Kiani R (Third Author), Methodologist/Assistant Researcher/Statistical Analyst (20%)
Funding: The present study was not financially supported.
One of the long-term consequences of increasing life expectancy and changing the age structure is the aging of the population. Population aging is inevitable for countries that have experienced mortality reduction and health and social development [1]. As a developing society, Iran is also facing this phenomenon. The increase in the elderly population is different from the growth of the population of other age groups, and recent evidence based on the 2016 census shows that the rate of growth has increased [2]. The elderly population of Iran aged 60 and above will increase from a little over 7.4 million people in 2016 to nearly 33.4 million people in 2056 [3]. In other words, until that year, more than a quarter of the country's population is made up of elderly people.
In the rural society of Iran, although life expectancy in villages is lower than in cities [4], due to high migration from rural to urban areas, especially rural youth migration, the proportion of the elderly population in rural areas is higher than in urban areas [5, 6]. For example, in 2011, based on the relative distribution of the population in terms of major age groups, 6.5% in rural areas and 5.4% in urban areas were in the age groups above 65 years, which shows the difference in the proportion of the elderly population in cities and villages [7].
Elderly issues are recognized as a research priority in developed countries to determine the psychological, social, and health needs of the elderly. But despite little attention in developing countries, there is a great need for research on various aspects of elderly people in these countries. Because the issue of old age, especially for the poor elderly in third-world countries, where welfare systems are less extensive, is a very important action [8].
In these countries, especially in Iran, people in society need formal and informal support from the government, social institutions, and people around them to achieve a better quality of life and solve their problems, especially in old age [9]. In traditional societies, social support during old age was provided by children, relatives, neighborhood members, and religious networks, respectively. Now, over time, the change in the function of the family in today's societies, the evolution of the family system from extended to the nuclear family, women's employment, etc. has led to a change in support patterns, and a part of the support that was provided by family and relatives in the past has now been transferred to official and defined institutions, such as government health care and private retirement organizations [10]. Therefore, considering the changes made in the Iranian society, especially the rural society, and also considering that most of the villagers are less covered by insurance due to the characteristics of the labor market in rural areas [6], the quality of life of the rural elderly has been affected [11], and in general the quality of life in villages is often lower [12].
The World Health Organization (WHO) defines quality of life as people's perception of their position in life based on the value systems and culture in which they live and in relation to their goals, expectations, standards, and concerns [8]. Also, in another definition, quality of life is defined as a concept with several domains, including mental and physical health, social functioning, and emotional/emotional well-being [13]. In general, it can be said that the quality of life is a multi-dimensional construct, consisting of the objective conditions of life and mental well-being [14, 15]. The objective dimension includes the apparent and tangible state of life, and the subjective dimension includes people's perceptions and values of their life situation [16]. It should be acknowledged that the quality of life and the possibility of a better life are strongly affected by time and place, and its components and factors change according to the time period and geographical location [14, 16].
Also, it seems that the elderly who live in the villages are at risk of reducing their quality of life compared to their counterparts in the cities due to the specific economic and social factors of the rural environment. These factors include geographic and social separation from the larger urban community, limited access to specialized care, and possibly lower socio-economic status [17]. Surveys also show that there are differences between urban and rural communities in access to quality of life indicators, and the quality of life of rural communities is in unfavorable conditions compared to urban residents [18].
Considering that Iran is one of the countries that has a large young population that will form the elderly population in the future [19], and as mentioned, the proportion of elderly people in villages is more than in cities, so it is necessary to pay attention to their quality of life. If proper planning is not implemented to take care of the physical, mental and social health of the elderly in rural areas, the society will face many problems in this field in the future [6]. Investigating the quality of life of rural elderly can be useful for recognizing, monitoring and evaluating previous policy strategies, designing future policies and plans, as well as identifying human priorities in life, causes of people's dissatisfaction, etc. [18]. In addition, most of the studies on the quality of life in Iran have been conducted in terms of location in urban areas and fewer have been addressed in rural areas [20], and in the case of rural elderly, it has been much less.
The review of the literature shows that to determine and measure the quality of life of the elderly in rural areas, it is necessary to pay attention to both subjective and objective dimensions, and three important dimensions, namely physical health, social and environmental functions, and emotional and mental well-being in the works of researchers such as Yazdanpour and Saam Aram [21], Baernholdt et al. [13], Alizadeh et al. [16] and Dongre and Deshmukh [22] have been considered.
Regarding the factors that determine the quality of life of the elderly in rural areas, the studies of Yazdanpour and Saam Aram [21], Hajihashemi et al. [17], Farhadi et al. [23], Rezvani et al. [24], Joshi et al. Dongre and Deshmukh [22], Banjare et al. [25] and Baernholdt et al. [13] have examined demographic variables as well as social and economic variables such as housing ownership status, level of communication with family members, support, participation, spiritual status, feeling of loneliness, income status, and such things.
This research aimed to investigate the quality of life of the rural elderly in the southern counties of Fars province (Lamard and Mehr counties) and the determining factors affecting it.
Instruments and Methods
The present research is a survey study. The research population was the elderly of Lamard and Mehr cities in the south of Fars province (12151 people aged 60 and above) in 2021. Based on Cochran's formula, the sample size for each city was calculated as 372 people. However, due to the geographical distribution of the region and the importance of the subject under study, the sample was increased to 825 people. Then, with the cluster sampling method, the target area was divided into 18 main blocks based on the number of rural districts. In the second stage, 4 blocks were selected from Lamard City and 3 blocks from Mehr City. Then, a number of villages were selected from the rural district (block) and finally, in a systematic way (based on the list of the health network of the rural district center of the population over 60 years old for each village), the target sample was selected, and data was collected.
The tool for collecting data in the survey is questionnaire. In addition to the demographic questions, the main part of the questionnaire was related to the measurement of the concepts of different aspects of the quality of life as well as its determinants. The World Health Organization Quality of Life (WHOQOL) was used to assess the dimensions of quality of life based on mental-psychological status, physical health, and social- environmental status. The concept of loneliness was measured according to the study of Zarghami and Mahmoudian [26]. In Zarghami and Mahmoudian's study, the feeling of loneliness was evaluated according to UCLA's modified loneliness scale, which includes 20 items, and its shorter 3-item form, as well as De Jong Gierveld Scale, which includes 11 items [26].
In addition to the descriptive statistics used to present a picture of the studied sample, to check the effect of different variables, and also the most important variable explaining the concept of quality of life, the step-by-step regression method was used.
Findings
Out of 825 people in the statistical sample, 43.3% were men, and 56.7% were women. The highest percentage of respondents was in the age group of 75 years and above, with 27.6% (227 people), followed by the age groups of 60-64, 65-69, and 70-74. About 19% (151 people) of the households were single-person households. Also, about 50% (397 people) of the families had more than 3 members.
In terms of marital status, approximately 32% (264 people) were without a spouse (death or divorce), and 67% (552 people) had a spouse and were living with their spouse. Only 1.5% (12 people) of the sample did not have children, and other elderly people had at least one child. Also, most of the elderly were illiterate (62%, 208 people), and the rest (32%, 107 people) had only literacy and elementary education.
Almost 80% stated that their living expenses are less than 1.5 million Tomans, and it seems that since about 90% (715 people) had housing, the lack of housing costs has a role in the low costs. Children and spouse (according to income from inherited land and household work) were the most important financial supporters.
20% (165 people) of the elderly expressed their feeling of loneliness much and very much. Also, 76% (627 people) of elderly people were satisfied with their health status.
Based on the physical health aspect, about 18% (148 people) of the elderly reported low quality of life, 37% average (305 people) and 45% (372 people) high. The mental-psychological dimension of quality of life was almost the same as the physical health dimension. Based on the social- environmental dimension, 35% (289 people) of people rated their quality of life low, and almost 48% (396 people) rated it high.
Physical dimension
The effect of the total independent variables of gender, age, number of family members, marital status, number of children, education, cost of living, housing condition, spirituality, feeling of loneliness, and the type of financial aid on the physical dimension of the quality of life of the elderly was investigated using the step-by-step regression method. In the first step, the cost of living variable was entered into the model as the most important variable. The coefficient of determination (R2) calculated from the first model showed that the cost of living explains 30% of the changes in the quality of life (physical dimension) as a dependent variable. Also, F=10.2 (p<0.01) showed that the independent variable (living expenses) entered in the first model is able to explain well the amount of changes and variance of the dependent variable. The beta regression coefficient and the t value, which determines the relative contribution of each independent variable and the significance of the effect in explaining changes in the dependent variable, indicated that the cost of living has the greatest role in predicting the dependent variable (Beta=-0.535). Therefore, the high cost of living has a negative effect on the quality of life of the elderly. In the second step, the spirituality variable had a positive effect on the quality of life of the elderly. By entering this variable, the coefficient of determination increased to 40%. In the next steps, feelings of loneliness, age, and education were entered into the model, and according to the fifth step, almost 60% of the changes in the dependent variable were explained. The variables of loneliness and age showed that the elderly who experience more loneliness and are older have a lower quality of life. The beta coefficients indicated that the cost of living and age variables have the greatest effect on the dependent variable. So, in general, the increase in living costs, age, and feeling of loneliness decrease the quality of life in the physical dimension, and education and spirituality increase it (Table 1).
Table 1) The effect of independent variables on the physical dimension of the quality of life of rural elderly in southern Fars
Mental-psychological dimension
The cost of living variable was entered as the first variable and explained 40% of the changes in the mental-psychological dimension of the quality of life. The beta regression coefficient and t value showed that living costs play the biggest role in predicting the dependent variable (Beta=-0.432). In the next steps, spirituality, feeling of loneliness, age, and education were entered into the model. The increase in living costs, feeling of loneliness, and age reduced the mental and psychological quality of life of the elderly, and spirituality and education had a positive effect on it. According to the fifth step, almost 60% of the dependent variable changes were explained. Beta coefficients indicated that the variables of living costs and age have the greatest effect on the dependent variable. In this way, the elderly, who have a higher cost of living and are at an older age, have a low quality of life in mental-psychological dimension (Table 2).
Social- environmental dimension
Variables were entered into the model in 9 steps. In the first step, the cost of living variable was entered into the model as the most important variable and had a negative effect on the social-environmental dimension of the quality of life of the elderly. The coefficient of determination of the first model showed that the cost of living explains 19% of the changes in the social-environmental dimension of the quality of life. In the next steps, spirituality, education, children's financial support, feelings of loneliness, spouse's financial support, age and housing ownership, and gender were entered into the model, respectively, and based on the ninth step, almost 64% of the changes in the dependent variable were explained. The beta coefficients indicated that the variable of spirituality has the highest effect, so that people who have higher spirituality also have a higher quality of life. Also, people who have a higher cost of living and feelings of loneliness and older have a lower quality of life. The financial support of children and spouses and the housing ownership also had a positive and significant effect on the social-environmental quality of life of the elderly. In this way, with the increase in living costs and feelings of loneliness, the quality of life in the social-environmental dimension decreases, and with the increase in spirituality, education, financial support, and the type of housing ownership, the quality of life of the elderly increases in the social-environmental dimension (Table 3).
Table 2) The effect of independent variables on the mentalpsychological dimension of the quality of life of rural elderly in southern Fars
Table 3) The effect of independent variables on the social-environmental dimension of the quality of life of rural elderly in southern Fars
Quality of life in general
Cost of living, housing ownership, spirituality, feeling of loneliness, number of children, gender, age, and education were entered into the model as influencing variables in 8 steps. The calculated R2 indicated that in the first step, the cost of living variable explained 28% of the changes in the dependent variable, and in the final step, all variables explained 59% of the changes in the dependent variable. In all steps, the F value showed the ability of independent variables in estimating the amount of changes and variance of the dependent variable. In step 8, cost of living, feelings of loneliness, and spirituality had the highest effect. The rising cost of living, age, and feelings of loneliness had a negative effect on the quality of life of the elderly, and housing ownership, high spirituality, having children, education, and being a man had a positive effect on the quality of life (Table 4).
Table 4) The effect of independent variables on the quality of life of rural elderly in southern Fars
Discussion
Research in the field of health and the welfare of the elderly is one of the fundamental issues in public health. Today, the elderly are becoming a significant part of the country's rural population, and this trend will continue to increase in the future. Therefore, it is necessary to identify their various needs, such as psychological, social, economic, and health needs, especially at the community level, to have the necessary planning and predictions for the future. By formulating and designing appropriate and practical policies and programs, the quality of life of the elderly and their satisfaction can be improved, and the problems that may arise in this field for different sectors, such as the health system, social system, economic system, etc., can be prevented. In this regard, examining the quality of life of the rural elderly determines their current life situation and helps to identify the determining factors to improve the effective factors and design better programs. With this perspective, in this research, the quality of life of the rural elderly and its determining factors were examined.
The results of this research showed that children and spouses were the most important financial supporters of the rural elderly. Also, about 80% of the elderly felt a little lonely, which shows that living in the village and communicating more with neighbors and relatives, as well as the continuous communication of children with their parents in rural environments, has an effect on the low level of this issue. In fact, family relationships and family support during old age play an effective role in improving the quality of life of the elderly.
One of the important goals of this research was to measure the quality of life of the rural elderly. About 45% of the elderly evaluated the quality of life in physical health and mental-psychological status as high. In the social-environmental dimension, about 48% had a high quality of life.
The results show that the elderly, who have high living expenses, experience more loneliness, and are older, have a lower quality of life in terms of physical and mental health. Also, education and spirituality have a positive effect on the quality of life of the elderly in these two dimensions, which is consistent with the study of Esmaeili and Esmaeili [27] and Jadidi et al. [28]. In the social-environmental dimension, the increase in living expenses and the feeling of loneliness decrease the quality of life, which is in line with the results of Zarghami and Mahmoudian's study [26], but spirituality, education, financial support of children and spouse's financial assistance, and the type of housing increase the quality of life of the elderly in this dimension.
In general, rising cost of living, age, and feeling of loneliness have a negative effect on the health and quality of life of the rural elderly, and housing, spirituality, financial support from children, education, and being a man have a positive effect on their health and quality of life.
Regarding the negative influencing factors on the quality of life of the elderly, the findings of this research about the cost of living in the works of Yazdanpour and Saam Aram [21] and Hajihashemi et al. [17], age in the works of Joshi et al. [8] and Hajihashemi et al. [17] and the feeling of loneliness in the works of Dongre and Deshmukh [22] and Baernholdt et al. [13] have been confirmed. Here it can be said that the two important variables of living costs and feeling of loneliness are the main findings of this work, and to change and improve the quality of life of the rural elderly, attention and policies in these two variables are necessary.
Regarding the cost of living, considering that the coverage of social security insurance and social welfare in the villages is low due to the working conditions of the villagers, it is necessary to pay more attention to the rural elderly, especially in the field of their health, and diagnostic-therapeutic and welfare services and facilities should be considered for them at lower or free rates, which means there is a need for an efficient support system. Regarding the feeling of loneliness, rural elderly may be socially isolated, and therefore, they need interventions to preserve physical and mental health and strengthen social relationships and support and increase participation in society.
Another issue that was investigated in this study was the positive influencing factors on the quality of life of the elderly. In line with the results of this study, the spirituality variable has been confirmed in the study of Dongre and Deshmukh [22], the financial support of children in the study of Yazdanpour and Saam Aram [21] and the ownership of housing in the study of Joshi et al. [8]. Considering the differences between urban and rural elderly in terms of education, income, access to health facilities [23], insurance coverage, etc., rural elderly are at lower levels of quality of life. Therefore, the economic dimensions and support of children are important in order to overcome these limitations and show the perspectives of intervention and design of suitable and practical policies and programs.
This study had some limitations because it was conducted among the elderly and in a rural community. It is difficult to obtain information and research data from elderly people, and people of this age are less willing to give information. In addition, elderly people's understanding of the subjects changes with every little issue that happens to them, which makes it more difficult to investigate the research topic. For example, if an elderly person faces foot pain or other problems the day before, this will quickly affect his/her other perceptions on various issues. Another point was the statistical population of elderly rural people, who were mostly illiterate or poorly educated, and the interviewer had to speak their local language and accent, which made the data collection process very long.
It is suggested to use qualitative methods and mixed methods to know the quality of life of the rural elderly. Also, for future research, a comparison can be made between the quality of life of rural and urban elderly.
According to the results of the present study, it is necessary to pay attention to the two factors of loneliness and living expenses of the rural elderly. It is also necessary to encourage and value the support of children from elderly parents and to think of ways to continue this relationship. Regarding the access of the elderly to housing in the villages, programs should also be planned.
Conclusion
Feeling of loneliness and cost of living are two important factors in reducing the quality of life and health of rural elderly. Also, the financial support of children and the acquisition of housing plays an important role in increasing the quality of life of the rural elderly.
Acknowledgements: The authors would like to acknowledge all the people who have collaborated in the preparation of data for this article.
Ethical Permission: The questionnaire used in this research has been approved by the scientific committee of Payam Noor University, Lamard Center.
Conflict of Interests: There is no conflict of interests.
Authors’ Contribution: Nobakht R (First Author), Introduction Writer/Methodologist/Main Researcher/Discussion Writer (50%); Rostamalizadeh V (Second Author), Methodologist/Assistant Researcher/Discussion Writer (30%); Kiani R (Third Author), Methodologist/Assistant Researcher/Statistical Analyst (20%)
Funding: The present study was not financially supported.
Keywords:
References
1. United Nations. World population ageing 2019: highlights. New York: United Nations; 2019. [Link]
2. Statistical Center of Iran. Results of the 2016 housing and population census [Internet]. Tehran: Statistical Center of Iran; 2015 [cited 2022 March 18]. Available from: https://www.amar.org.ir [Persian] [Link]
3. Zanjari N, Sadeghi R. Iran's old age watch index in 2016. 1st Edition. Tehran: Saba Pension Strategies Institute; 2020. [Persian] [Link]
4. Kousheshi M. Life tables of the country in 2015 based on the statistics of death registration in Iran. Tehran: Insurance Research Center (Iran); 2018. [Persian] [Link]
5. Mirzaei M, Shams Ghahfarokhi M. Demography of elder population in Iran over the period 1956 to 2006. Salmand. 2007;2(3):326-31. [Persian] [Link]
6. Pahlevanzadeh F, Jarollahi O. Analysis of the effect of social factors on mental health of rural elderlies. J Community Dev. 2011;3(1):65-84. [Persian] [Link]
7. Statistical Center of Iran. Results of the 2011 housing and population census [Internet]. Tehran: Statistical Center of Iran; 2011 [cited 2022 March 18]. Available from: https://www.amar.org.ir [Persian] [Link]
8. Joshi MR, Chalise HN, Khatiwada PP. Quality of life of Nepalese elderly living in rural Nepal. J Gerontol Geriatr Res. 2018;7(5):1-6. [Link]
9. Zanjari N, Sani MS, Chavoshi MH, Rafiey H, Shahboulaghi FM. Successful aging as a multidimensional concept: An integrative review. Med J Islam Repub Iran. 2017;31:100. [Link] [DOI:10.14196/mjiri.31.100]
10. Mousavi M, Mostafaei A. Analyzing life quality of retired elderly in Tehran (Focusing on formal and informal social support). Soc Dev Welfare Plann. 2011;3(7):137-64. [Persian] [Link]
11. Rezvani M, Mansourian H, Ahmadadadi H, Ahmadabadi F, Parvai Here-Dasht S. An assessment on factors affecting the quality of life of elderly in rural regions (Case study: Neishabour County). J Rural Res. 2013;4(2):301-26. [Persian] [Link]
12. Soroshmehr H, Azami M, Yaghobi A, Mehreghan N. Analysis of quality of rural life in Iran using Fuzzy method. Soc Welfare Q. 2017;17(65):69-102. [Persian] [Link]
13. Baernholdt M, Yan G, Hinton I, Rose K, Mattos M. Quality of life in rural and urban adults 65 years and older: findings from the National Health and Nutrition Examination survey. J Rural Health. 2012;28(4):339-47. [Link] [DOI:10.1111/j.1748-0361.2011.00403.x]
14. Coulthard S, Johnson D, McGregor A. Poverty, sustainability and human wellbeing: A social wellbeing approach to the global fisheries crisis. J Glob Environ Change. 2011;21(2):453-63. [Link] [DOI:10.1016/j.gloenvcha.2011.01.003]
15. Michalska-Żyła A, Marks-Krzyszkowska M. Quality of life and quality of living in rural communes in Poland. European Countryside. 2018;10(2):280-99. [Link] [DOI:10.2478/euco-2018-0017]
16. Alizadeh J, Barghi H, Rahimi H, Afsharipour A. Evaluating quality of life in rural areas using Fuzzy Topsis. Case Study: Myandeh Village, Fars Province. J Rural Res. 2013;4(3):615-40. [Persian] [Link]
17. Hajihashemi Z, Vameghi R, Montazeri A, Sohrabi MR, Akbari-Kamrani A. Comparing quality of life among rural and urban elderly outpatients. Payesh. 2013;12(3):255-62. [Persian] [Link]
18. Jamini D, Safari Aliakbari M, Salahi Kakhaki M, Alipoor K, Zolfaghari A. Spatial distribution of quality of life and identification of its determinants in rural settlements (Case study: Ravansar County in Kermanshah Province). Geograph Environ Plann. 2017;28(2):57-78. [Persian] [Link]
19. Mohebbi L, Zahednejad S, Javadi Pour S, Saki A. Domestic elder abuse in rural area of Dezful, Iran and its relation with their quality of life. Salmand. 2016;10(4):50-9. [Persian] [Link]
20. Badri A, Rezvani M, Gharanjik M. The quality of life measurement in rural areas based on subjective indicators. Case study: Sothern Jafarby Dehestan, Torkman County. Geograph Environ Plann. 2013;24(2):53-74. [Persian] [Link]
21. Yazdanpour F, Saam Aram E. Effective factors on life quality of elderly in Khomein. Soc Dev Welfare Plann. 2011;3(6):45-64. [Persian] [Link]
22. Dongre AR, Deshmukh PR. Social determinants of quality of elderly life in a rural setting of India. Indian J Palliat Care. 2012;18(3):181-9. [Link] [DOI:10.4103/0973-1075.105688]
23. Farhadi A, Foroughan M, Mohammadi F. The quality of life among rural elderlies. A cross-sectional study. Salmand. 2011;6(2):38-46. [Persian] [Link]
24. Rezvani M R, Parvaei S, Mansouriyan H. Assessment of effective factors on the elder quality of life in urban areas in Neishabour and Ashgabat. Geograph Urban Space Dev. 2015;2(1):39-55. [Link]
25. Banjare P, Dwivedi R, Pradhan J. Factors associated with the life satisfaction amongst the rural elderly in Odisha, India. Health Qual Life Outcomes. 2015;13:1-201. [Link] [DOI:10.1186/s12955-015-0398-y]
26. Zarghami H, Mahmoudian H. Children's out-migration and loneliness feeling in rural older parents. Health Psychol. 2016;19(5):99-116. [Persian] [Link]
27. Esmaeili R, Esmaeii M. Quality of life in the elderly: A meta-synthesis. J Res Relig Healh. 2018;4(2):105-16. [Persian] [Link]
28. Jadidi A, Farhanian M, Janmohammadi S, Haghani H. The relationship between spiritual well-being and quality of life among elderly people residing in Kahrizak Senior House. Iran J Nurs. 2011;24(72):48-56. [Persian] [Link]