
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

1.0
Cite Score 2025
SJR: 0.129 / SNIP: 0.140
Volume 14, Issue 4 (2022)
Iran J War Public Health 2022, 14(4): 361-366 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2022/06/29 | Accepted: 2022/10/10 | Published: 2022/11/1
Received: 2022/06/29 | Accepted: 2022/10/10 | Published: 2022/11/1
How to cite this article
Eslahi H, Karajibani M, Payandeh A, Montazerifar F. Eating Behaviors and Food Habits of Veterans; A Case Study in Zahedan City. Iran J War Public Health 2022; 14 (4) :361-366
URL: http://ijwph.ir/article-1-1194-en.html
URL: http://ijwph.ir/article-1-1194-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:


1- Department of Nutrition, School of Medicine, Zahedan University of Medical Sciences, Zahedan, Iran
2- “Health Promotion Research Center” and “Department of Nutrition, School of Medicine”, Zahedan University of Medical Sciences, Zahedan, Iran
3- “Infectious Diseases and Tropical Medicine Research Center” and “Resistant Tuberculosis Institute”, Zahedan University of Medical Sciences, Zahedan, Iran
4- “Pregnancy Health Research Center” and “Department of Nutrition, School of Medicine”, Zahedan University of Medical Sciences, Zahedan, Iran
2- “Health Promotion Research Center” and “Department of Nutrition, School of Medicine”, Zahedan University of Medical Sciences, Zahedan, Iran
3- “Infectious Diseases and Tropical Medicine Research Center” and “Resistant Tuberculosis Institute”, Zahedan University of Medical Sciences, Zahedan, Iran
4- “Pregnancy Health Research Center” and “Department of Nutrition, School of Medicine”, Zahedan University of Medical Sciences, Zahedan, Iran
Full-Text (HTML) (1122 Views)
Introduction
The ever-increasing changes in lifestyle and food patterns cause health problems and death in various vulnerable groups, which puts different groups of society at risk with the spread of chronic diseases in developing and developed countries [1]. Healthy eating and lifestyle habits are required to improve the well-being of people [2]. Inappropriate diets, along with a lack of physical inactivity, increase the risk for obesity, heart disease, and Type 2 Diabetes (T2DM) [3]. Food behaviors have a broad concept and this process with the food choices made have significant consequences in terms of lifestyle and continuity of health for the individual and society [4]. Nutritional behaviors are influenced by many factors, such as food availability, food preferences, portion sizes or food rations, cultural values, family beliefs, food processing, and storage. Experience and social teachings can change behaviors and eating habits [5]. Nutritional habits are an influential indicator of eating and drinking behavior. It includes a set of various nutritional functions related to food selection, preparation and serving [6]. The main factors affecting the adoption of healthy or unhealthy eating habits include beliefs, genetic factors, and environmental factors that interact with each other and have different effects [7].
Modifying one’s eating behaviors is an important step toward preventing non-communicable diseases as well as reducing and controlling disease complications. In this context, nutrition education is an effective practical method to promote nutritional knowledge, public awareness, and public health [8]. Nutritional knowledge can have significant effects on selecting a healthy and nutritious diet [9]. In addition, inappropriate nutritional knowledge is a major factor influencing nutritional problems and can influence dietary practices [10]. Proper nutritional attitudes and beliefs of the community significantly improve healthy eating [11].
Among people, optimal dietary intake is essential for veterans and the military environment due to their physical and mental requirements [12, 13]. Malnutrition is associated with higher mortality rates in veterans [14, 15], in particular in the elderly [16], and food insecurity affects the low diet quality in veterans [16-18]. They are also at risk for overweight and obesity compared to other people and may experience increased rates of eating disorders [19]. Studies have reported rates of 32.70% obesity [20] and 33.90% [21] among veterans. It was reported that the obesity rate was 12.00% higher in veterans compared with service members, which highlights military separation as a high risk for being overweight [22]. In overweight and obese veterans, low fruit and vegetable consumption is often associated with tobacco use [23]. Unhealthy dietary and lifestyle habits, including smoking, are common in veterans [24-26], increasing the risk of cancer and Cardiovascular Diseases (CVD) [27]. It was reported that demographic risk factors, trauma, and the military environment increase the risk for veterans [28]. The incidence of trauma increases in eating disorders in veterans [19].
Bankoff et al. investigated eating behavior in male veterans and showed that veterans may experience eating disorder and food addiction symptoms [29]. Cuthbert et al. studied eating disorders in veterans, which could lead to overweight and obesity [28].
Veterans are a special group which suffer from physical, therapeutic, mental, and psychological problems that can lead to inability to continue living. Therefore, it is important to study various aspects of their health, such as eating habits and nutritional literacy and behaviors. Therefore, this study aimed to evaluate eating habits and behaviors in veterans of Zahedan.
Instruments and Methods
This cross-sectional study was conducted on all veterans from 19 February 2021 to 21 June 2021 in Zahedan city. The statistical population included 2000 veterans, and 322 veterans were selected based on the following formula:
The above formula suggested a sample size of 322 participants. However, we finalized the sample size at 369 individuals to account for possible attrition.
Data collection
Data were collected using three questionnaires; 1) Demographic information, 2) Eating habits, and 3) Nutritional behaviors.
Demographic information: Demographic characteristics included age, job, education, married status, weight, height and Body Mass Index (BMI), having a percentage of veterans, and family size. According BMI index, participants were categorized as underweight, normal weight, overweight, and obese.
Eating habits: Eating habits were recorded by a questionnaire comprising 12 questions. This questionnaire was provided to the veterans, and the results were expressed in the number and percentage of each question.
Nutritional behaviors: Nutritional behaviors including nutritional knowledge, attitude, and practices were evaluated. The data for nutritional knowledge were collected by a questionnaire with 11 questions that scored based on 0 as false and 1 as true. A total knowledge score of 19-26, 12-18, and less than 12 indicated good, moderate, and weak knowledge, respectively. The data for nutritional attitude were collected by a questionnaire with 6 questions, which classified as agreement (2), disagreement (0) and lack of opinion (1). A total attitude score of 9-12, 5-8, and 0-4 represented good, moderate, and weak attitude, respectively. Also, the data for nutritional practice were collected by a questionnaire with 10 questions that scored based on 0 as false and 1 as true. A total practice score of 12-15, 7-11, and less than 7 represented good, moderate, and weak practice, respectively.
Statically analysis
Data were presented as mean±SD and distribution frequency. Statistical analysis was performed by SPSS 21 software. Pearson's correlation coefficient and chi-square test were used to determine the relationship between variables. P-value <0.05 was considered statistically significant.
Findings
The mean age of the participants was 48.40±11.37 years, the mean body weight was 74.75±13.00 kg, the mean height was 174.50±8.87 cm, the mean BMI was 24.52±3.72 kg/m2, and the mean of family size was 2.10, respectively. Based on literacy level, 60 people (16.3%) had preliminary education, 135 people (36.6%) had high school education, 142 people (38.5%) had academic education, and 32 people (8.7%) were illiterate. In terms of occupation, 36 people (9.8%) were housewives, 36 people (9.8%) were retired, 72 people (19.5%) were workers, 163 people (44.2%) were employees, and 62 people (16.8%) were free-lancers. Most veterans (n=347, 94%) were married, and the rest were single (n=22, 6%).
The most participants consumed 3 meals. 35.2% consumed no salt foods, and 49.1% consumed medium-salt foods. Most veterans fried potato and eggplant as well as vegetables in golden or roast forms. The most intake oil was liquid or frying oils. They mostly stored meat and meat processes raw. The majority of participants drank tea and coffee as lukewarm and watery foods in warmish form. Most of the water and bread storage containers were also plastic (Table 1).
The cooking utensils used by 158 people (42.8%) were Teflon, and 82 people (22.2%) were copper. Other materials of cooking utensils included zinc (n=20, 5.4%), aluminum (n=49, 13.3%), enamel (n=16, 4.3%), cast iron (n=13, 3.5%), steel (n=13, 3.5%), Pyrex (n=6, 1.6%), and others (n=12, 3.3%).
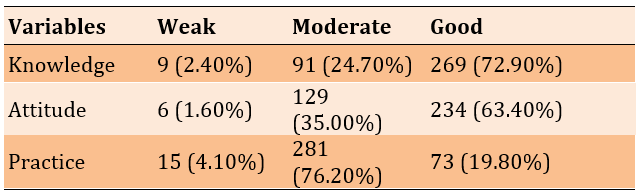
The mean scores of nutritional knowledge, attitude, and practice of the participants were 16.31±2.97, 9.2±2.32, and 10.23±2.61, respectively. 72.90%, 63.40%, and 19.80% of nutritional knowledge, attitude, and practices were in good status, respectively. In terms of practice, most of them had a moderate status (Table 2).
Table 1) Frequency distribution of eating habits of the participants
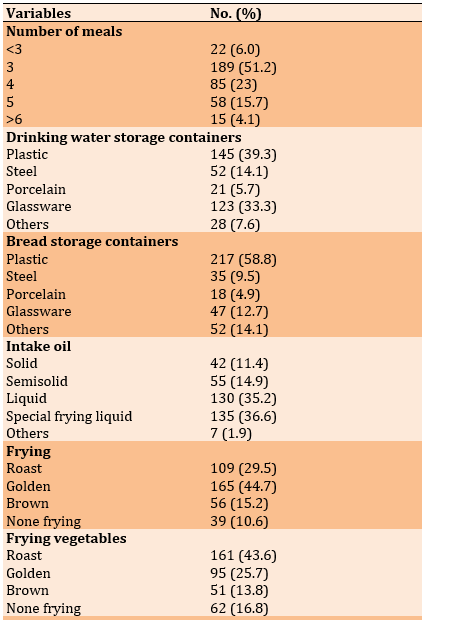
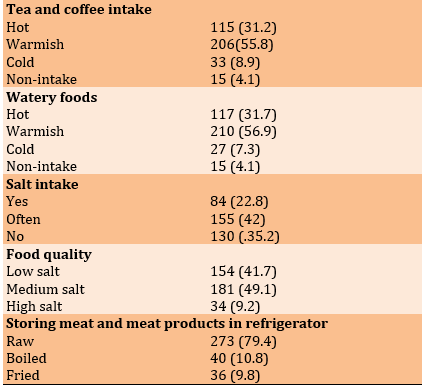
Table 2) The frequency distribution of nutritional knowledge, attitude and practices in participants
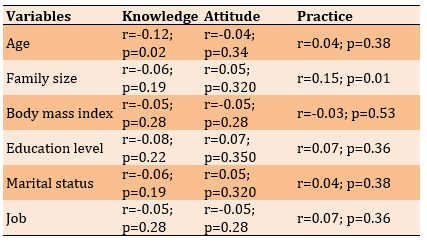
There was a negative significant correlation between age and knowledge (r=- 0.12; p=0.02) and a positive significant correlation between family size and practice (r=0.15, p=0.01). No significant correlation was observed between other demographic variables with knowledge, attitude and practice (Table 3).
Table 3) Correlation between demographic variables with nutritional knowledge, attitude and practice in participants
Discussion
This study aimed to investigate the eating behaviors and food habits of veterans in Zahedan city. Our findings showed that the studied people were middle-aged with a normal BMI. Most participants were an employee and had a diploma and academic education.
The present study showed that most participants consumed 3 meals (51.20%). A positive correlation between the number of meals received and improvement in body composition was reported [30]. Most participants used salty foods. Several studies have reported the adverse effects of salty foods on health [31, 32]. It seems veterans must consider a special program for decreasing salt consumption. Based on findings, most veterans fried potato, eggplant, and also vegetables in golden and roast forms. It was reported that roasting conditions can increase deliciousness and healthiness via protecting antioxidants [33]. However, modifying their daily diet seems necessary. Thus, most veterans selected an appropriate procedure for frying potatoes, eggplant, and vegetables. In addition, liquid and frying oils are mostly utilized for frying. Oils with a significant amount of double bonds and free fatty acids are prone to oxidation. However, consuming liquid oil and frying oil decrease serum lipid levels and help to improve healthiness [34]. Most participants usually stored meat in raw form (80.0%). Freezing meat and meat processes help to maintain nutrient values, while cooking and storing may cause interactions that result in decreased nutrient values. The veterans mostly consumed tea, coffee, and watery foods in warmish form. Hot drinks and foods may damage the digestive tract, and thus consumption of warmish foods helps to improve freshness and healthiness. In addition, most containers for storing bread and water were plastic. The application of plastic containers may be a challenge because these may threaten healthiness [35]. Thus, they must consider cautious aspects. The cooking dishes were almost copper and aluminum. These dishes may release trace elements into foods and cause toxicity that must be considered cautious aspects during food cooking and should not be used constantly.
Our findings also showed that participants had a desirable status for knowledge and attitude while they had a moderate condition for practices. The results are consistent with previous studies for infection prevention [36, 37] and cardiovascular disease prevention [38] in the study population. However, increasing knowledge was negatively associated with increasing age. Older people may not accept updated information and only accept traditional systems. Knowledge of nutrition has a positive effect on selecting healthy and nutritious diets [9]. The results confirm that elderly veterans may need educational programs to improve their knowledge. Knowledge has a closed relation with practice.
The logical action theory emphasizes the association between beliefs, attitudes, and behaviors. Modification of knowledge and attitude improves behavior.
Inappropriate nutritional knowledge is a major factor influencing nutritional problems and can influence dietary practices [10]. In addition, our results confirmed non-significant relation between family size, BMI, education levels, married status, and job with knowledge. In addition, our findings showed that attitude did not have any relation with demographic characteristics. Understanding the nutritional attitude and beliefs of the community significantly improve healthy eating [11]. The result of the present study is not in agreement with previous studies that showed a significant relationship between attitude and education levels [39, 40]. It seems the differences could be attributed to education levels in the studied population in the current study and previous studies; because the most studied people had an academic education level. The results also showed a negative relationship between practice level and family size.
It is suggested to implement supplementary, participatory, and advisory programs to improve the nutrition practice of veterans. It is also recommended to use the capacity of households and local facilities in addition to education and nutritional support programs. More studies are needed to understand the factors affecting KAP in participants.
This study was conducted on veterans in Zahedan city and cannot be interpreted for all populations. The limitations of this study include the small number of samples and its cross-sectional nature, which hindered the temporal evaluation of the results. It was difficult to conclude a basic relationship between different factors concerning the aim of the study. Hence, more studies with a larger sample size should be conducted in modifying the lifestyle of the studied community. It is recommended that more extensive studies be conducted on larger populations and with longer follow-ups to obtain more conclusive results.
Conclusion
The veterans of the study use suitable and acceptable methods in the processing of different foods, including the use of liquid oil and stored meat. Nevertheless, they also consume salty foods and use more plastic containers. The level of their knowledge and attitude is appropriate, but the level of practice in the participants is not optimal. There is a negative correlation between age and knowledge level that needs to be considered a nutritional intervention program in the following target group. However, poor levels of practice are observed. Considering the relationship between indicators including knowledge, attitude, and practice suggests that improving the nutritional awareness of the participants can help to modify their attitude and consequently, their practice.
Acknowledgment: We would like to thank all the participants in this study for their conscientious contribution and thank the colleagues who willingly contributed to this research.
Ethical Permission: This research was approved by the Ethics Committee of Martyr Foundation and Veterans Affairs with financial assistants Registration No. IR.ISSAR.REC.1401.004.
Conflicts of interest: The authors declare that they have no conflicts of interest.
Authors’ Contribution: Eslahi H. (First author), Introduction author/Discussion author (30%); Karajibani M. (Second author), Methodologist/Original researcher (40%); Payandeh A. (Third author), Statistical analyst (15%); Montazerifar F. (Fourth author), Assistant (15%)
Funding: This research was done with the financial support of the Martyr Foundation and Veterans Affairs.
The ever-increasing changes in lifestyle and food patterns cause health problems and death in various vulnerable groups, which puts different groups of society at risk with the spread of chronic diseases in developing and developed countries [1]. Healthy eating and lifestyle habits are required to improve the well-being of people [2]. Inappropriate diets, along with a lack of physical inactivity, increase the risk for obesity, heart disease, and Type 2 Diabetes (T2DM) [3]. Food behaviors have a broad concept and this process with the food choices made have significant consequences in terms of lifestyle and continuity of health for the individual and society [4]. Nutritional behaviors are influenced by many factors, such as food availability, food preferences, portion sizes or food rations, cultural values, family beliefs, food processing, and storage. Experience and social teachings can change behaviors and eating habits [5]. Nutritional habits are an influential indicator of eating and drinking behavior. It includes a set of various nutritional functions related to food selection, preparation and serving [6]. The main factors affecting the adoption of healthy or unhealthy eating habits include beliefs, genetic factors, and environmental factors that interact with each other and have different effects [7].
Modifying one’s eating behaviors is an important step toward preventing non-communicable diseases as well as reducing and controlling disease complications. In this context, nutrition education is an effective practical method to promote nutritional knowledge, public awareness, and public health [8]. Nutritional knowledge can have significant effects on selecting a healthy and nutritious diet [9]. In addition, inappropriate nutritional knowledge is a major factor influencing nutritional problems and can influence dietary practices [10]. Proper nutritional attitudes and beliefs of the community significantly improve healthy eating [11].
Among people, optimal dietary intake is essential for veterans and the military environment due to their physical and mental requirements [12, 13]. Malnutrition is associated with higher mortality rates in veterans [14, 15], in particular in the elderly [16], and food insecurity affects the low diet quality in veterans [16-18]. They are also at risk for overweight and obesity compared to other people and may experience increased rates of eating disorders [19]. Studies have reported rates of 32.70% obesity [20] and 33.90% [21] among veterans. It was reported that the obesity rate was 12.00% higher in veterans compared with service members, which highlights military separation as a high risk for being overweight [22]. In overweight and obese veterans, low fruit and vegetable consumption is often associated with tobacco use [23]. Unhealthy dietary and lifestyle habits, including smoking, are common in veterans [24-26], increasing the risk of cancer and Cardiovascular Diseases (CVD) [27]. It was reported that demographic risk factors, trauma, and the military environment increase the risk for veterans [28]. The incidence of trauma increases in eating disorders in veterans [19].
Bankoff et al. investigated eating behavior in male veterans and showed that veterans may experience eating disorder and food addiction symptoms [29]. Cuthbert et al. studied eating disorders in veterans, which could lead to overweight and obesity [28].
Veterans are a special group which suffer from physical, therapeutic, mental, and psychological problems that can lead to inability to continue living. Therefore, it is important to study various aspects of their health, such as eating habits and nutritional literacy and behaviors. Therefore, this study aimed to evaluate eating habits and behaviors in veterans of Zahedan.
Instruments and Methods
This cross-sectional study was conducted on all veterans from 19 February 2021 to 21 June 2021 in Zahedan city. The statistical population included 2000 veterans, and 322 veterans were selected based on the following formula:
The above formula suggested a sample size of 322 participants. However, we finalized the sample size at 369 individuals to account for possible attrition.
Data collection
Data were collected using three questionnaires; 1) Demographic information, 2) Eating habits, and 3) Nutritional behaviors.
Demographic information: Demographic characteristics included age, job, education, married status, weight, height and Body Mass Index (BMI), having a percentage of veterans, and family size. According BMI index, participants were categorized as underweight, normal weight, overweight, and obese.
Eating habits: Eating habits were recorded by a questionnaire comprising 12 questions. This questionnaire was provided to the veterans, and the results were expressed in the number and percentage of each question.
Nutritional behaviors: Nutritional behaviors including nutritional knowledge, attitude, and practices were evaluated. The data for nutritional knowledge were collected by a questionnaire with 11 questions that scored based on 0 as false and 1 as true. A total knowledge score of 19-26, 12-18, and less than 12 indicated good, moderate, and weak knowledge, respectively. The data for nutritional attitude were collected by a questionnaire with 6 questions, which classified as agreement (2), disagreement (0) and lack of opinion (1). A total attitude score of 9-12, 5-8, and 0-4 represented good, moderate, and weak attitude, respectively. Also, the data for nutritional practice were collected by a questionnaire with 10 questions that scored based on 0 as false and 1 as true. A total practice score of 12-15, 7-11, and less than 7 represented good, moderate, and weak practice, respectively.
Statically analysis
Data were presented as mean±SD and distribution frequency. Statistical analysis was performed by SPSS 21 software. Pearson's correlation coefficient and chi-square test were used to determine the relationship between variables. P-value <0.05 was considered statistically significant.
Findings
The mean age of the participants was 48.40±11.37 years, the mean body weight was 74.75±13.00 kg, the mean height was 174.50±8.87 cm, the mean BMI was 24.52±3.72 kg/m2, and the mean of family size was 2.10, respectively. Based on literacy level, 60 people (16.3%) had preliminary education, 135 people (36.6%) had high school education, 142 people (38.5%) had academic education, and 32 people (8.7%) were illiterate. In terms of occupation, 36 people (9.8%) were housewives, 36 people (9.8%) were retired, 72 people (19.5%) were workers, 163 people (44.2%) were employees, and 62 people (16.8%) were free-lancers. Most veterans (n=347, 94%) were married, and the rest were single (n=22, 6%).
The most participants consumed 3 meals. 35.2% consumed no salt foods, and 49.1% consumed medium-salt foods. Most veterans fried potato and eggplant as well as vegetables in golden or roast forms. The most intake oil was liquid or frying oils. They mostly stored meat and meat processes raw. The majority of participants drank tea and coffee as lukewarm and watery foods in warmish form. Most of the water and bread storage containers were also plastic (Table 1).
The cooking utensils used by 158 people (42.8%) were Teflon, and 82 people (22.2%) were copper. Other materials of cooking utensils included zinc (n=20, 5.4%), aluminum (n=49, 13.3%), enamel (n=16, 4.3%), cast iron (n=13, 3.5%), steel (n=13, 3.5%), Pyrex (n=6, 1.6%), and others (n=12, 3.3%).
The mean scores of nutritional knowledge, attitude, and practice of the participants were 16.31±2.97, 9.2±2.32, and 10.23±2.61, respectively. 72.90%, 63.40%, and 19.80% of nutritional knowledge, attitude, and practices were in good status, respectively. In terms of practice, most of them had a moderate status (Table 2).
Table 1) Frequency distribution of eating habits of the participants
Table 2) The frequency distribution of nutritional knowledge, attitude and practices in participants
There was a negative significant correlation between age and knowledge (r=- 0.12; p=0.02) and a positive significant correlation between family size and practice (r=0.15, p=0.01). No significant correlation was observed between other demographic variables with knowledge, attitude and practice (Table 3).
Table 3) Correlation between demographic variables with nutritional knowledge, attitude and practice in participants
Discussion
This study aimed to investigate the eating behaviors and food habits of veterans in Zahedan city. Our findings showed that the studied people were middle-aged with a normal BMI. Most participants were an employee and had a diploma and academic education.
The present study showed that most participants consumed 3 meals (51.20%). A positive correlation between the number of meals received and improvement in body composition was reported [30]. Most participants used salty foods. Several studies have reported the adverse effects of salty foods on health [31, 32]. It seems veterans must consider a special program for decreasing salt consumption. Based on findings, most veterans fried potato, eggplant, and also vegetables in golden and roast forms. It was reported that roasting conditions can increase deliciousness and healthiness via protecting antioxidants [33]. However, modifying their daily diet seems necessary. Thus, most veterans selected an appropriate procedure for frying potatoes, eggplant, and vegetables. In addition, liquid and frying oils are mostly utilized for frying. Oils with a significant amount of double bonds and free fatty acids are prone to oxidation. However, consuming liquid oil and frying oil decrease serum lipid levels and help to improve healthiness [34]. Most participants usually stored meat in raw form (80.0%). Freezing meat and meat processes help to maintain nutrient values, while cooking and storing may cause interactions that result in decreased nutrient values. The veterans mostly consumed tea, coffee, and watery foods in warmish form. Hot drinks and foods may damage the digestive tract, and thus consumption of warmish foods helps to improve freshness and healthiness. In addition, most containers for storing bread and water were plastic. The application of plastic containers may be a challenge because these may threaten healthiness [35]. Thus, they must consider cautious aspects. The cooking dishes were almost copper and aluminum. These dishes may release trace elements into foods and cause toxicity that must be considered cautious aspects during food cooking and should not be used constantly.
Our findings also showed that participants had a desirable status for knowledge and attitude while they had a moderate condition for practices. The results are consistent with previous studies for infection prevention [36, 37] and cardiovascular disease prevention [38] in the study population. However, increasing knowledge was negatively associated with increasing age. Older people may not accept updated information and only accept traditional systems. Knowledge of nutrition has a positive effect on selecting healthy and nutritious diets [9]. The results confirm that elderly veterans may need educational programs to improve their knowledge. Knowledge has a closed relation with practice.
The logical action theory emphasizes the association between beliefs, attitudes, and behaviors. Modification of knowledge and attitude improves behavior.
Inappropriate nutritional knowledge is a major factor influencing nutritional problems and can influence dietary practices [10]. In addition, our results confirmed non-significant relation between family size, BMI, education levels, married status, and job with knowledge. In addition, our findings showed that attitude did not have any relation with demographic characteristics. Understanding the nutritional attitude and beliefs of the community significantly improve healthy eating [11]. The result of the present study is not in agreement with previous studies that showed a significant relationship between attitude and education levels [39, 40]. It seems the differences could be attributed to education levels in the studied population in the current study and previous studies; because the most studied people had an academic education level. The results also showed a negative relationship between practice level and family size.
It is suggested to implement supplementary, participatory, and advisory programs to improve the nutrition practice of veterans. It is also recommended to use the capacity of households and local facilities in addition to education and nutritional support programs. More studies are needed to understand the factors affecting KAP in participants.
This study was conducted on veterans in Zahedan city and cannot be interpreted for all populations. The limitations of this study include the small number of samples and its cross-sectional nature, which hindered the temporal evaluation of the results. It was difficult to conclude a basic relationship between different factors concerning the aim of the study. Hence, more studies with a larger sample size should be conducted in modifying the lifestyle of the studied community. It is recommended that more extensive studies be conducted on larger populations and with longer follow-ups to obtain more conclusive results.
Conclusion
The veterans of the study use suitable and acceptable methods in the processing of different foods, including the use of liquid oil and stored meat. Nevertheless, they also consume salty foods and use more plastic containers. The level of their knowledge and attitude is appropriate, but the level of practice in the participants is not optimal. There is a negative correlation between age and knowledge level that needs to be considered a nutritional intervention program in the following target group. However, poor levels of practice are observed. Considering the relationship between indicators including knowledge, attitude, and practice suggests that improving the nutritional awareness of the participants can help to modify their attitude and consequently, their practice.
Acknowledgment: We would like to thank all the participants in this study for their conscientious contribution and thank the colleagues who willingly contributed to this research.
Ethical Permission: This research was approved by the Ethics Committee of Martyr Foundation and Veterans Affairs with financial assistants Registration No. IR.ISSAR.REC.1401.004.
Conflicts of interest: The authors declare that they have no conflicts of interest.
Authors’ Contribution: Eslahi H. (First author), Introduction author/Discussion author (30%); Karajibani M. (Second author), Methodologist/Original researcher (40%); Payandeh A. (Third author), Statistical analyst (15%); Montazerifar F. (Fourth author), Assistant (15%)
Funding: This research was done with the financial support of the Martyr Foundation and Veterans Affairs.
References
1. World Health Organization. Diet, nutrition and the prevention of chronic diseases. World Health Organ Tech Rep Ser. 2003;916(i-viii):1-149. [Link]
2. Bawaked RA, Gomez SF, Homs C, Esteve RC, Cardenas G, Fíto M, et al. Association of eating behaviors, lifestyle, and maternal education with adherence to the Mediterranean diet in Spanish children. Appetite. 2018;130:279-85. [Link] [DOI:10.1016/j.appet.2018.08.024]
3. Reicks M, Banna J, Cluskey M, Gunther C, Hongu N, Richards R, et al. Influence of parenting practices on eating behaviors of early adolescents during independent eating occasions: implications for obesity prevention. Nutrients. 2015;7(10):8783-801. [Link] [DOI:10.3390/nu7105431]
4. Hurt RT, Kulisek C, Buchanan LA, McClave SA. The obesity epidemic: challenges, health initiatives, and implications for gastroenterologists. Gastroenterol Hepatol. 2010;6(12):780-92. [Link]
5. Jessica Osorio E, Gerardo Weistaubb N, Carlos Castillo D. Development of feeding behavior in childhood and its alterations. Revista Chilena de Nutrición. 2002;29(3):280-5. [Spanish] [Link] [DOI:10.4067/S0717-75182002000300002]
6. Domínguez-Vásquez P, Olivares S, Santos J. Eating behavior and childhood obesity: family influences. Arch Latinoam Nutr. 2008;58(3):249-55. [Spanish] [Link]
7. Çelik ÇB, Odacı H, Bayraktar N. Is problematic internet use an indicator of eating disorders among Turkish university students? Eat Weight Disord. 2015;20(2):167-72. [Link] [DOI:10.1007/s40519-014-0150-3]
8. Makiabadi E, Kaveh MH, Mahmoodi MR, Asadollahi A, Salehi M. Enhancing nutrition-related literacy, knowledge and behavior among university students: a randomized controlled trial. Int J Nutr Sci. 2019;4(3):122-9. [Link]
9. Worsley A. Nutrition knowledge and food consumption: can nutrition knowledge change food behaviour? Asia Pac J Clin Nutr. 2002;11 Suppl 3:S579-85. [Link] [DOI:10.1046/j.1440-6047.11.supp3.7.x]
10. Ul Haq I, Mariyam Z, Li M, Huang X, Jiang P, Zeb F, et al. A comparative study of nutritional status, knowledge attitude and practices (KAP) and dietary intake between international and Chinese students in Nanjing, China. Int J Environ Res Public Health. 2018;15(9):1910. [Link] [DOI:10.3390/ijerph15091910]
11. Kearney JM, Gibney MJ, Livingstone BE, Robson PJ, Kiely M, Harrington K. Attitudes towards and beliefs about nutrition and health among a random sample of adults in the Republic of Ireland and Northern Ireland. Public Health Nutr. 2001;4(5A):1117-26. [Link] [DOI:10.1079/PHN2001193]
12. Barringer ND, Pasiakos SM, McClung HL, Crombie AP, Margolis LM. Prediction equation for estimating total daily energy requirements of special operations personnel. J Int Soc Sports Nutr. 2018;15:15. [Link] [DOI:10.1186/s12970-018-0219-x]
13. McAdam JS, McGinnis KD, Beck DT, Haun CT, Romero MA, Mumford PW, et al. Effect of whey protein supplementation on physical performance and body composition in army initial entry training soldiers. Nutrients. 2018;10(9):1248. [Link] [DOI:10.3390/nu10091248]
14. Hiller LD, Shaw RF, Fabri PJ. Difference in composite end point of readmission and death between malnourished and nonmalnourished veterans assessed using academy of nutrition and dietetics/american society for parenteral and enteral nutrition clinical characteristics. J Parenter Enteral Nutr. 2017;41(8):1316-24. [Link] [DOI:10.1177/0148607116668523]
15. Win AZ, Ceresa C, Arnold K, Allison T. High prevalence of malnutrition among elderly veterans in home based primary care. J Nutr Health Aging. 2017;21(6):610-3. [Link] [DOI:10.1007/s12603-017-0918-z]
16. O'Toole TP, Roberts CB, Johnson EE. Peer reviewed: screening for food insecurity in six veterans administration clinics for the homeless, June-December 2015. Prev Chronic Dis. 2017;14:E04. [Link] [DOI:10.5888/pcd14.160375]
17. Becerra MB, Hassija CM, Becerra BJ. Food insecurity is associated with unhealthy dietary practices among US veterans in California. Public Health Nutr. 2017;20(14):2569-76. [Link] [DOI:10.1017/S1368980016002147]
18. Miller DP, Larson MJ, Byrne T, DeVoe E. Food insecurity in veteran households: findings from nationally representative data. Public Health Nutr. 2016;19(10):1731-40. [Link] [DOI:10.1017/S1368980015003067]
19. Bartlett BA, Mitchell KS. Eating disorders in military and veteran men and women: A systematic review. Int J Eat Disord. 2015;48(8):1057-69. [Link] [DOI:10.1002/eat.22454]
20. Stefanovics EA, Potenza MN, Pietrzak RH. The physical and mental health burden of obesity in US veterans: Results from the National Health and Resilience in Veterans Study. J Psychiatr Res. 2018;103:112-9. [Link] [DOI:10.1016/j.jpsychires.2018.05.016]
21. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA. 2010;303(3):235-41. [Link] [DOI:10.1001/jama.2009.2014]
22. Rush T, LeardMann CA, Crum‐Cianflone NF. Obesity and associated adverse health outcomes among US military members and veterans: findings from the millennium cohort study. Obesity. 2016;24(7):1582-9. [Link] [DOI:10.1002/oby.21513]
23. Ko LK, Allicok M, Campbell MK, Valle CG, Armstrong-Brown J, Carr C, et al. An examination of sociodemographic, health, psychological factors, and fruit and vegetable consumption among overweight and obese US veterans. Mil Med. 2011;176(11):1281-6. [Link] [DOI:10.7205/MILMED-D-11-00021]
24. Hoerster KD, Wilson S, Nelson KM, Reiber GE, Masheb RM. Diet quality is associated with mental health, social support, and neighborhood factors among Veterans. Eat Behav. 2016;23:168-73. [Link] [DOI:10.1016/j.eatbeh.2016.10.003]
25. Park S-Y, Zhu K, Potter JF, Kolonel LN. Health-related characteristics and dietary intakes of male veterans and non-veterans in the Multiethnic Cohort Study (United States). J Mil Veterans Health. 2011;19(2):4. [Link]
26. Tessier JM, Erickson ZD, Meyer HB, Baker MR, Gelberg HA, Arnold IY, et al. Therapeutic lifestyle changes: impact on weight, quality of life, and psychiatric symptoms in veterans with mental illness. Mil Med. 2017;182(9-10):e1738-44. [Link] [DOI:10.7205/MILMED-D-16-00405]
27. Sai XY, He Y, Men K, Wang B, Huang JY, Shi QL, et al. All-cause mortality and risk factors in a cohort of retired military male veterans, Xi'an, China: an 18-year follow up study. BMC Public Health. 2007;7(1):290. [Link] [DOI:10.1186/1471-2458-7-290]
28. Cuthbert K, Hardin S, Zelkowitz R, Mitchell K. Eating disorders and overweight/obesity in veterans: Prevalence, risk factors, and treatment considerations. Curr Obes Rep. 2020;9(2):98-108. [Link] [DOI:10.1007/s13679-020-00374-1]
29. Bankoff SM, Richards LK, Bartlett B, Wolf EJ, Mitchell KS. Examining weight and eating behavior by sexual orientation in a sample of male veterans. Compr Psychiatry. 2016;68:134-9. [Link] [DOI:10.1016/j.comppsych.2016.03.007]
30. Schoenfeld BJ, Aragon AA, Krieger JW. Effects of meal frequency on weight loss and body composition: a meta-analysis. Nutr Rev. 2015;73(2):69-82. [Link] [DOI:10.1093/nutrit/nuu017]
31. Kongstad S, Giacalone D. Consumer perception of salt-reduced potato chips: Sensory strategies, effect of labeling and individual health orientation. Food Qual Prefer. 2020;81:103856. [Link] [DOI:10.1016/j.foodqual.2019.103856]
32. Newson R, Elmadfa I, Biro G, Cheng Y, Prakash V, Rust P, et al. Barriers for progress in salt reduction in the general population. An international study. Appetite. 2013;71:22-31. [Link] [DOI:10.1016/j.appet.2013.07.003]
33. Tomita H, Uchida K, Takemori T, editors. Cooking research on deliciousness and healthiness: Texture analysis on cooked rice using SEM images and anti-oxidant capacity of roasted vegetables. International Gas :union: Research Conference. Denmark; 2014. [Link]
34. Mohammadifard N, Nazem M, Naderi G-A, Saghafian F, Sajjadi F, Maghroon M, et al. Effect of hydrogenated, liquid and ghee oils on serum lipids profile. ARYA Atheroscler. 2010;6(1):16-22. [Link]
35. Bou-Mitri C, Abdessater M, Zgheib H, Akiki Z. Food packaging design and consumer perception of the product quality, safety, healthiness and preference. Nutr Food Sci. 2021;51(1):71-86. [Link] [DOI:10.1108/NFS-02-2020-0039]
36. Sinkowitz-Cochran RL, Burkitt KH, Cuerdon T, Harrison C, Gao S, Obrosky DS, et al. The associations between organizational culture and knowledge, attitudes, and practices in a multicenter Veterans Affairs quality improvement initiative to prevent methicillin-resistant Staphylococcus aureus. Am J Infect Control. 2012;40(2):138-43. [Link] [DOI:10.1016/j.ajic.2011.04.332]
37. Burkitt KH, Sinkowitz-Cochran RL, Obrosky DS, Cuerdon T, Miller LJ, Jain R, et al. Survey of employee knowledge and attitudes before and after a multicenter Veterans' Administration quality improvement initiative to reduce nosocomial methicillin-resistant Staphylococcus aureus infections. Am J Infect Control. 2010;38(4):274-82. [Link] [DOI:10.1016/j.ajic.2009.08.019]
38. Kazemi T, Bijari B. Knowledge, attitude and performance of Birjand city veterans and their wives about cardiovascular diseases risk factors. Iran J War Public Health. 2014;6(3):95-100. [Link]
39. Sajjadi F, MohammadiFard N, Khosravi A, Bahonar A, Maghroon M, Fathi M, et al. Nutritional knowledge attitude and practice of health professionals about cardiovascular diseases. J Birjand Univ Med Sci. 2008;15(2):65-72. [Persian] [Link]
40. Salahshoori A, Nasirzadeh M, Haruni J, Pourhaji F, Salahshoori S, Nozarpoor J. The knowledge, attitude, and practice (KAP) of Women Health Services Staff about risk factors of cardiovascular diseases (CVDs) in city of Fereydan and Chadegan, Iran. Jundishapur J Chronic Dis Care. 2015;4(1):1-5. [Link] [DOI:10.5812/jjcdc.26599]