
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

0.4
Cite Score
SJR: 0.114 / SNIP: 0.090
Volume 13, Issue 3 (2021)
Iran J War Public Health 2021, 13(3): 221-228 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2021/08/25 | Accepted: 2021/11/17 | Published: 2022/01/1
Received: 2021/08/25 | Accepted: 2021/11/17 | Published: 2022/01/1
How to cite this article
Ghiyasi Noei A, Sabahi P, Rafieinia P. Effectiveness of Unified Transdiagnostic Therapy on Cognitive Emotion Regulation, Experimental Avoidance and Post-Traumatic Stress Disorder in Veterans. Iran J War Public Health 2021; 13 (3) :221-228
URL: http://ijwph.ir/article-1-1000-en.html
URL: http://ijwph.ir/article-1-1000-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Department of Psychology, Faculty of Educational Sciences and Psychology, Semnan University, Semnan, Iran
Full-Text (HTML) (937 Views)
Introduction
Surviving a war while other friends are dying or seriously injured is one of life's most painful experiences, which can lead to physical, cognitive, and emotional reactions [1]. Post-Traumatic Stress Disorder (PTSD) was first introduced in the American Psychiatric Association Diagnostic Classification in 1980 [2]. It is estimated that 90% of people are exposed to traumatic events at least once in their lifetime. However, not everyone develops PTSD after a traumatic event [3]. In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), PTSD symptoms include disturbing symptoms (formerly re-experienced), avoidance symptoms, and negative changes in cognition, mood, and arousal [4]. Each symptom has adverse effects on the individual, interpersonal, and social aspects.
One of the reasons that people suffer from psychological problems is emotional causes. It has been shown that people with PTSD have many difficulties in cognitive emotion regulation [5]. Emotion regulation refers to determining what emotion to experience and express at what time [6]. Cognitive emotion regulation refers to the processes of information and managing emotional reactions when facing negative events [7]. In other words, cognitive emotion regulation strategies are patterns of reaction to exciting events. A reaction can be conscious or unconscious, and its purpose is to modify or correct the intensity and type of emotional experience of a person [8]. Mclean et al. found that cognitive distortions and cognitive emotion regulation strategies are two important mediators in PTSD [9]. Also, dysfunctional emotional, cognitive regulation is associated with more severe PTSD symptoms. In another study, Kelly et al. showed that difficulty in emotionally cognitive regulation could predict PTSD symptoms in war survivors. The problems in regulating emotion could manifest as excessive aggravation or reduction of excitement and cause people to use inefficient methods such as obsessive rumination, catastrophizing, and overeating facing excitement [10]. These dysfunctional coping patterns may temporarily reduce arousal, making emotional coping more difficult [11].
Emotion regulation is conducted in different ways, whereas recent meta-analytic research shows that experiential avoidance is one of the main methods and is considered a strategy in PTSD psychiatric pathology [12]. Williams et al. stated that PTSD is associated with experiential avoidance, especially in people with high sensitivity to the behavioral inhibition system [1]. Experience avoidance is the process by which a person is reluctant to engage in painful experiences, hence seeking to control, suppress, and curb the thoughts, feelings, and behaviors related to the negative events [13]. This process can have the opposite effect on reducing anxiety for people who experience a traumatic event. So, people with PTSD, instead of experiencing and reprocessing thoughts and feelings by avoiding them intensify and perpetuate the anxiety [2]. Evidence suggests that if PTSD is not treated, the sufferer is at risk for many psychiatric problems such as depression, neuropsychological disorders, memory impairment, emotion regulation, physical health problems, reduced resilience, and problems adapting to family and couples [14]. PTSD also leads to high costs for military personnel [15]. Therefore, the treatment of these people is important.
One of the effective treatments for these people is integrated transdiagnostic therapy. The initial version of unified transdiagnostic therapy was used by Ellard et al. [16] for a heterogeneous sample of emotional disorders. Transdiagnostic therapy treats emotional disorders by combining therapeutic components. Transdiagnostic therapy focuses specifically on improving emotion regulation skills [16]. In other words, the emphasis is on emotions’ adaptive and functional nature in this treatment. It is mainly an attempt to modify non-adaptive efforts to regulate emotional experiences and facilitate appropriate processing [17]. García-Escalera et al., in a study examining the effectiveness of an integrated protocol in emotional disorders in young people, concluded that transdiagnostic therapy has a significant effect on the reduction of emotional disorders [18]. Sawiris and Berl conducted 15 studies on 1,244 people. The results showed significant anxiety, depression, generalized anxiety disorder, obsessive-compulsive disorder, social anxiety, agoraphobia, and borderline personality disorder. They also showed that unified transdiagnostic therapy helps to improve emotion regulation strategies [19]. Basharpoor et al. concluded that the effect of transdiagnostic therapy is significantly higher in people with the obsessive-compulsive disorder compared to exposure therapy and response prevention in improving experiential avoidance and cognitive emotion regulation [2]. Fadaei et al. concluded that Barlow's unified transdiagnostic therapy protocol increased differentiation in the experimental group compared to the control group and reduced the difficulty level of emotion regulation [21]. Osmani and Shukri stated that unified transdiagnostic therapy significantly affected students' cognitive emotion regulation and cognitive empathy with an externalized behavior disorder. The effect of unified transdiagnostic therapy was 72 and 67% on students' cognitive emotion regulation and cognitive empathy with an externalized behavior disorder, respectively [22].
Since few studies have investigated the effect of transdiagnostic therapy on the components of cognitive emotion regulation and experimental avoidance in patients with PTSD, this study aimed to evaluate the effectiveness of unified transdiagnostic therapy on cognitive emotion regulation, experimental avoidance, and diagnostic symptoms of post-traumatic stress disorder in veterans.
Materials and Methods
This was a quasi-experimental study with a two-group design of experiments and controls with pre-test and post-test, which was carried out on all veterans with post-traumatic stress disorder in Mashhad in 2020-2021. Thirty-two people were selected using G.power software 3.1.9.4 (based on effect size: 0.25, confidence level: 0.05, statistical power: 0.8, and several dependent variables: 3 and groups: 2) and randomly assigned to two 16-person experimental and control groups. Inclusion criteria included age range 55-70 years, 50-70% disability rate (due to problems that people with 50-70% injury rate), diagnosis of PTSD by the relevant specialist and having at least a diploma and being married.
The measurement tools were as follows:
1- Cognitive Emotion Regulation Questionnaire developed by Garnefski et al. [23]; It is a self-reported multidimensional questionnaire with 36 items and special forms for adults and children. In this questionnaire, the person is asked to indicate his/her reaction in the face of threatening experiences and stressful events (by answering five questions that evaluate the strategy for controlling and regulating emotion) [7]. The questionnaire is scored on the 5-point Likert scale; never (1), rarely (2), sometimes (3), often (4), and always (5). This questionnaire comprises single positive focus/planning, positive evaluation/a broader perspective, self-blame, blaming others, rumination, catastrophizing, and acceptance. The alpha coefficient for subscales has been reported in 0.71 to 0.81 [23]. The Persian version of this questionnaire has been validated in Iran [24]. The convergent and divergent validity of this form was also examined by Issazadegan and Fatehabad in Iran [25].
In the present study, Cronbach's alpha for the subscales of self-blame, blame others, catastrophe, rumination, acceptance, positive focus, and positive evaluation were equal to 0.72, 0.74, 0.69, 0.75, 0.77, 0.82, and 0.77, respectively.
2- Experimental Avoidance Questionnaire developed by Gámez et al. The questionnaire included 62 items and evaluated six subscales of behavioral avoidance, incompatible distress, postponement, distraction/suppression, denial/suppression, and distress tolerance by 6-point Likert scale from strongly agree=5 to strongly disagree=0. Questions 23 and 30 are scored in reverse [26]. Gámez et al. reported Cronbach's alpha coefficients in different samples from 0.91 to 0.95 and the correlation of this instrument with the Commitment and Practice Questionnaire (r=0.74) as an indicator of appropriate validity. Cronbach's alpha coefficients for the subscales of behavioral avoidance, incompatible distress, postponement, distraction/suppression, denial/suppression, and tolerance of disaster were 0.77, 0.70, 0.55, 0.80, 0.78, and 0.79, respectively. In the present study, Cronbach's alpha for the instrument was 0.82.
3- The post Traumatic Stress Disorder Questionnaire is a self-reported scale with 20 items developed by Weathers et al. for evaluation of PTSD diagnostic criteria in DSM-5. This questionnaire assesses four scales of harassment, avoidance, negative changes in mood and cognition, and excessive arousal, which 5, 2, 7, and 6 items are related to the signs of re-experiencing a traumatic event, avoidance, negative changes in cognition, and mood, and arousal, respectively. The scoring method of this questionnaire includes the sum of scores (0-80) obtained by the scores sum of 20 items based on a 5-point Likert scale. The cutting point is determined to be 38. Convergent validity in the English version of this questionnaire is reported to be 0.89 [27], and Talebigi has translated and standardized it and reported its reliability with Cronbach's alpha of 0.77 [28]. In the present study, Cronbach's alpha was 0.73.
4- An unified transdiagnostic therapy protocol has been developed by Barlow et al. and typically performs during 12 sessions [29].
The Ethical permission was obtained from the Postgraduate Education Council of the Faculty of Psychology of Semnan University. The implementation method was that the researcher referred to the Martyr Foundation of Mashhad. After justifying and presenting the questionnaires, the researcher was introduced to the support departments of each Martyr Foundation in the areas of Mashhad city. Then, the questionnaires were provided to the subjects with the cooperation of the support department, and it was decided that everyone who was referred to this ward would be given a post-traumatic stress disorder questionnaire for initial diagnosis and screening for PTSD. Then, those who were eligible were selected. After obtaining the subject’s consent to participate in the treatment, 32 people were selected by available sampling and were randomly divided into experimental and control groups. The intervention was performed by the first author in twelve 90-minutes sessions on Tuesdays at the Ryan Mehr Golshan Clinic in Mashhad. The intervention procedure lasted three months. The pre-test was performed after screening in the first intervention session, and the post-test was performed in the last session. Also, due to the prevalence of the Covid-19 virus, interventions were performed in person and following health protocols. Also, all ethical principles were observed, including confidentiality and obtaining a consent form. To control the effect of the intervention, the experimental and control groups did not interact during the intervention.
After data collection, data were analyzed at two descriptive (mean, standard deviation, frequency, and percentage) and at the inferential levels (multivariate analysis of covariance) using SPSS 23 software.
Surviving a war while other friends are dying or seriously injured is one of life's most painful experiences, which can lead to physical, cognitive, and emotional reactions [1]. Post-Traumatic Stress Disorder (PTSD) was first introduced in the American Psychiatric Association Diagnostic Classification in 1980 [2]. It is estimated that 90% of people are exposed to traumatic events at least once in their lifetime. However, not everyone develops PTSD after a traumatic event [3]. In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), PTSD symptoms include disturbing symptoms (formerly re-experienced), avoidance symptoms, and negative changes in cognition, mood, and arousal [4]. Each symptom has adverse effects on the individual, interpersonal, and social aspects.
One of the reasons that people suffer from psychological problems is emotional causes. It has been shown that people with PTSD have many difficulties in cognitive emotion regulation [5]. Emotion regulation refers to determining what emotion to experience and express at what time [6]. Cognitive emotion regulation refers to the processes of information and managing emotional reactions when facing negative events [7]. In other words, cognitive emotion regulation strategies are patterns of reaction to exciting events. A reaction can be conscious or unconscious, and its purpose is to modify or correct the intensity and type of emotional experience of a person [8]. Mclean et al. found that cognitive distortions and cognitive emotion regulation strategies are two important mediators in PTSD [9]. Also, dysfunctional emotional, cognitive regulation is associated with more severe PTSD symptoms. In another study, Kelly et al. showed that difficulty in emotionally cognitive regulation could predict PTSD symptoms in war survivors. The problems in regulating emotion could manifest as excessive aggravation or reduction of excitement and cause people to use inefficient methods such as obsessive rumination, catastrophizing, and overeating facing excitement [10]. These dysfunctional coping patterns may temporarily reduce arousal, making emotional coping more difficult [11].
Emotion regulation is conducted in different ways, whereas recent meta-analytic research shows that experiential avoidance is one of the main methods and is considered a strategy in PTSD psychiatric pathology [12]. Williams et al. stated that PTSD is associated with experiential avoidance, especially in people with high sensitivity to the behavioral inhibition system [1]. Experience avoidance is the process by which a person is reluctant to engage in painful experiences, hence seeking to control, suppress, and curb the thoughts, feelings, and behaviors related to the negative events [13]. This process can have the opposite effect on reducing anxiety for people who experience a traumatic event. So, people with PTSD, instead of experiencing and reprocessing thoughts and feelings by avoiding them intensify and perpetuate the anxiety [2]. Evidence suggests that if PTSD is not treated, the sufferer is at risk for many psychiatric problems such as depression, neuropsychological disorders, memory impairment, emotion regulation, physical health problems, reduced resilience, and problems adapting to family and couples [14]. PTSD also leads to high costs for military personnel [15]. Therefore, the treatment of these people is important.
One of the effective treatments for these people is integrated transdiagnostic therapy. The initial version of unified transdiagnostic therapy was used by Ellard et al. [16] for a heterogeneous sample of emotional disorders. Transdiagnostic therapy treats emotional disorders by combining therapeutic components. Transdiagnostic therapy focuses specifically on improving emotion regulation skills [16]. In other words, the emphasis is on emotions’ adaptive and functional nature in this treatment. It is mainly an attempt to modify non-adaptive efforts to regulate emotional experiences and facilitate appropriate processing [17]. García-Escalera et al., in a study examining the effectiveness of an integrated protocol in emotional disorders in young people, concluded that transdiagnostic therapy has a significant effect on the reduction of emotional disorders [18]. Sawiris and Berl conducted 15 studies on 1,244 people. The results showed significant anxiety, depression, generalized anxiety disorder, obsessive-compulsive disorder, social anxiety, agoraphobia, and borderline personality disorder. They also showed that unified transdiagnostic therapy helps to improve emotion regulation strategies [19]. Basharpoor et al. concluded that the effect of transdiagnostic therapy is significantly higher in people with the obsessive-compulsive disorder compared to exposure therapy and response prevention in improving experiential avoidance and cognitive emotion regulation [2]. Fadaei et al. concluded that Barlow's unified transdiagnostic therapy protocol increased differentiation in the experimental group compared to the control group and reduced the difficulty level of emotion regulation [21]. Osmani and Shukri stated that unified transdiagnostic therapy significantly affected students' cognitive emotion regulation and cognitive empathy with an externalized behavior disorder. The effect of unified transdiagnostic therapy was 72 and 67% on students' cognitive emotion regulation and cognitive empathy with an externalized behavior disorder, respectively [22].
Since few studies have investigated the effect of transdiagnostic therapy on the components of cognitive emotion regulation and experimental avoidance in patients with PTSD, this study aimed to evaluate the effectiveness of unified transdiagnostic therapy on cognitive emotion regulation, experimental avoidance, and diagnostic symptoms of post-traumatic stress disorder in veterans.
Materials and Methods
This was a quasi-experimental study with a two-group design of experiments and controls with pre-test and post-test, which was carried out on all veterans with post-traumatic stress disorder in Mashhad in 2020-2021. Thirty-two people were selected using G.power software 3.1.9.4 (based on effect size: 0.25, confidence level: 0.05, statistical power: 0.8, and several dependent variables: 3 and groups: 2) and randomly assigned to two 16-person experimental and control groups. Inclusion criteria included age range 55-70 years, 50-70% disability rate (due to problems that people with 50-70% injury rate), diagnosis of PTSD by the relevant specialist and having at least a diploma and being married.
The measurement tools were as follows:
1- Cognitive Emotion Regulation Questionnaire developed by Garnefski et al. [23]; It is a self-reported multidimensional questionnaire with 36 items and special forms for adults and children. In this questionnaire, the person is asked to indicate his/her reaction in the face of threatening experiences and stressful events (by answering five questions that evaluate the strategy for controlling and regulating emotion) [7]. The questionnaire is scored on the 5-point Likert scale; never (1), rarely (2), sometimes (3), often (4), and always (5). This questionnaire comprises single positive focus/planning, positive evaluation/a broader perspective, self-blame, blaming others, rumination, catastrophizing, and acceptance. The alpha coefficient for subscales has been reported in 0.71 to 0.81 [23]. The Persian version of this questionnaire has been validated in Iran [24]. The convergent and divergent validity of this form was also examined by Issazadegan and Fatehabad in Iran [25].
In the present study, Cronbach's alpha for the subscales of self-blame, blame others, catastrophe, rumination, acceptance, positive focus, and positive evaluation were equal to 0.72, 0.74, 0.69, 0.75, 0.77, 0.82, and 0.77, respectively.
2- Experimental Avoidance Questionnaire developed by Gámez et al. The questionnaire included 62 items and evaluated six subscales of behavioral avoidance, incompatible distress, postponement, distraction/suppression, denial/suppression, and distress tolerance by 6-point Likert scale from strongly agree=5 to strongly disagree=0. Questions 23 and 30 are scored in reverse [26]. Gámez et al. reported Cronbach's alpha coefficients in different samples from 0.91 to 0.95 and the correlation of this instrument with the Commitment and Practice Questionnaire (r=0.74) as an indicator of appropriate validity. Cronbach's alpha coefficients for the subscales of behavioral avoidance, incompatible distress, postponement, distraction/suppression, denial/suppression, and tolerance of disaster were 0.77, 0.70, 0.55, 0.80, 0.78, and 0.79, respectively. In the present study, Cronbach's alpha for the instrument was 0.82.
3- The post Traumatic Stress Disorder Questionnaire is a self-reported scale with 20 items developed by Weathers et al. for evaluation of PTSD diagnostic criteria in DSM-5. This questionnaire assesses four scales of harassment, avoidance, negative changes in mood and cognition, and excessive arousal, which 5, 2, 7, and 6 items are related to the signs of re-experiencing a traumatic event, avoidance, negative changes in cognition, and mood, and arousal, respectively. The scoring method of this questionnaire includes the sum of scores (0-80) obtained by the scores sum of 20 items based on a 5-point Likert scale. The cutting point is determined to be 38. Convergent validity in the English version of this questionnaire is reported to be 0.89 [27], and Talebigi has translated and standardized it and reported its reliability with Cronbach's alpha of 0.77 [28]. In the present study, Cronbach's alpha was 0.73.
4- An unified transdiagnostic therapy protocol has been developed by Barlow et al. and typically performs during 12 sessions [29].
The Ethical permission was obtained from the Postgraduate Education Council of the Faculty of Psychology of Semnan University. The implementation method was that the researcher referred to the Martyr Foundation of Mashhad. After justifying and presenting the questionnaires, the researcher was introduced to the support departments of each Martyr Foundation in the areas of Mashhad city. Then, the questionnaires were provided to the subjects with the cooperation of the support department, and it was decided that everyone who was referred to this ward would be given a post-traumatic stress disorder questionnaire for initial diagnosis and screening for PTSD. Then, those who were eligible were selected. After obtaining the subject’s consent to participate in the treatment, 32 people were selected by available sampling and were randomly divided into experimental and control groups. The intervention was performed by the first author in twelve 90-minutes sessions on Tuesdays at the Ryan Mehr Golshan Clinic in Mashhad. The intervention procedure lasted three months. The pre-test was performed after screening in the first intervention session, and the post-test was performed in the last session. Also, due to the prevalence of the Covid-19 virus, interventions were performed in person and following health protocols. Also, all ethical principles were observed, including confidentiality and obtaining a consent form. To control the effect of the intervention, the experimental and control groups did not interact during the intervention.
After data collection, data were analyzed at two descriptive (mean, standard deviation, frequency, and percentage) and at the inferential levels (multivariate analysis of covariance) using SPSS 23 software.
Table 1) Unified transdiagnostic therapy protocol of Barlow et al. [29]

Findings
The mean age of the experimental and control groups were 54.68±4.18 and 56.18±3.88, respectively. There wasn't a significant difference between the average age of the two groups (p<0.05). In the experimental group, 5, 8, and 3 subjects had a diploma and high school (31.30%), master (50%), and (18.70%) bachelor's degrees.
In the control group, 5, 5, and 6 subjects had a diploma, high school (31.30%), master (31.30%), and (37.40%) bachelor's degrees, respectively. Unified transdiagnostic therapy in the experimental group reduced self-blame, rumination, blaming others, catastrophizing, and increased acceptance and positive refocus. Positive re-evaluation compared to the control group who did not use this method. Also, in the experimental group, this therapy method reduced behavioral avoidance, incompatibility anxiety, postponements, distraction, and denial, and increased anxiety tolerance compared to the control group who did not use this method.
The therapy in the experimental group was able to reduce harassment, avoidance, negative mood changes, and extreme arousal compared to the control group who did not use this method (Table 2).
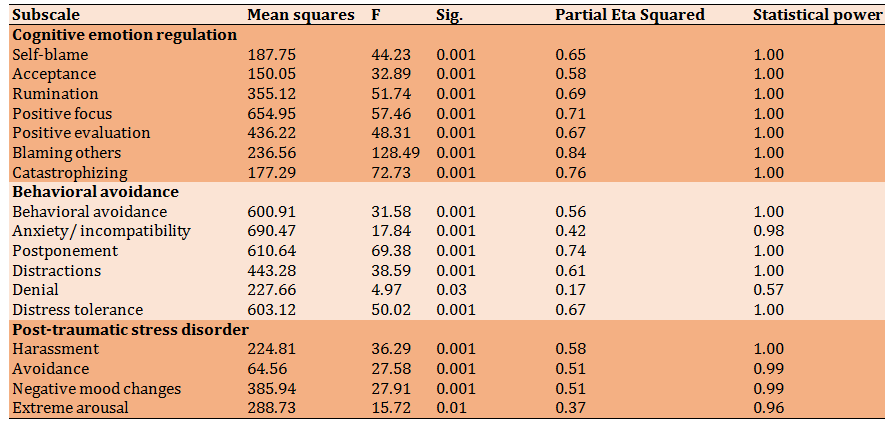
Before testing the hypotheses, the statistical hypotheses of multivariate and univariate analysis of covariance were examined. The results of Box's M test showed the homogeneity assumption of the variance-covariance matrix (p<0.19, F=9.75), which showed that the covariance matrices of the dependent variable are equal for the levels of the independent variable. Bartlett's sphericity test also showed that the correlation between dependent variables is sufficient to continue the analysis (p<0.001, Chi-square=15.48).
Based on the Leuven test, the homogeneity of variances in the total score of positive cognitive emotion regulation (p<0.23, F=0.12), negative cognitive regulation (p<0.96, F=0.08), and behavioral avoidance (p<0.080, F=0.06) were Observed, but in PTSD (p<0.01, F=6.74) the homogeneity assumption of variances was not observed. Also, the results of Lambda Wilkes and T. Hotline showed a significant difference in the linear composition of the research variables between the experimental and control groups in the post-test stage.
There was a significant difference between all components of cognitive emotion regulation, experimental avoidance, and diagnostic symptoms of PTSD in the experimental and control groups (Table 3).
Table 2) Mean±SD of the variables of control and experimental groups in veterans with 50-70% disability
rating in Mashhad city (n=32)
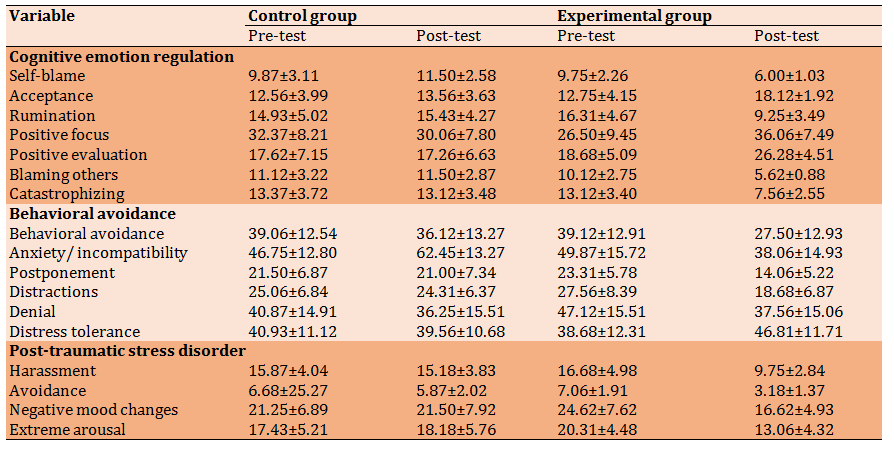
Table 3) Results of multivariate analysis of variance to investigate the differences between the experimental and control groups concerning the components of cognitive emotion regulation, experimental avoidance, and PTSD in veterans with 50-70% disability rating in Mashhad city (n=32)
Discussion
This study aimed to evaluate the effectiveness of unified transdiagnostic therapy on veterans' cognitive emotion regulation, experimental avoidance, and diagnostic symptoms of PTSD. The results showed that in the cognitive regulation of emotion, the experimental group scored lower than the control group in their components of self-blame, rumination, blaming others, and catastrophizing. The experimental group scored higher than the control group in the components of acceptance, positive refocus, and positive re-evaluation. Thus, unified transdiagnostic therapy reduced self-blame, rumination, blaming others, and catastrophizing in the experimental group, and increased acceptance, positive refocus, and positive re-evaluation. These findings follow several studies [19, 21, 31].
Emotion regulation is by which people consciously determine what emotion to experience and express at what time. Emotion regulation is consciously determining what emotion to experience and express at what time and how information is processed, and the individual responds facing a traumatic event, affecting people’s reactions. In other words, cognitive emotion regulation strategies are patterns of responding to exciting events. The response can be conscious or unconscious, and its purpose is to modify or correct the intensity and type of emotional experience of the individual. These dysfunctional coping patterns may temporarily reduce arousal, but it makes emotional coping more difficult [7].
The results showed that the experimental group had lower scores in the components of behavioral avoidance, anxiety, incompatibility, postponement,
distraction, and denial than the control group and higher scores in anxiety tolerance. Indeed, unified transdiagnostic therapy in the experimental group reduced behavioral avoidance, incompatibility anxiety, postponement, distraction, and denial and increased anxiety tolerance compared to the control group. Also, in the diagnostic symptoms of PTSD, the experimental group scored lower than the control group in the components of harassment, avoidance, negative mood changes, and extreme arousal. This result means that unified transdiagnostic therapy in the experimental group was able to reduce harassment, avoidance, negative mood changes, and extreme arousal compared to the control group who did not use this method, and these results are consistent with the results of several studies [16, 18, 20, 22]. In explaining the obtained results, it can be said that PTSD is associated with a high level of the functional defect and has a significant impact on the quality of life after trauma. Cognitive avoidance is considered a strategy in PTSD psychiatric pathology. PTSD is associated with experiential avoidance, especially in people with high levels of behavioral inhibition. As a strategy to reduce anxiety coping traumatic events, this process has the opposite effect. In this way, people with PTSD, instead of experiencing and reprocessing thoughts and feelings, aggravate and perpetuate anxiety by avoiding emotions.
On the other hand, unified transdiagnostic therapy can effectively improve cognitive regulation of emotion and cognitive avoidance in these individuals. Transdiagnostic therapy focuses specifically on improving emotion regulation skills. In other words, the emphasis of this therapy is on the adaptive and functional nature of emotions. It is mainly an attempt to modify non-adaptive efforts to regulate emotional experiences and facilitate appropriate processing. In transdiagnostic approaches, emotional experience and reaction are among the basic processes in psychological trauma, especially in emotional disorders [17].
The present study was carried out on veterans; war survivors show higher rates of trauma and PTSD [32], which may be due to their experience in war operations. In studies to identify the effects of war, the findings suggest that people with PTSD have problems developing social relationships and expressing emotions [14]. They also differ in impulse control, aggression, and marital problems from the general population. These problems prevent sufferers from playing their roles properly as parents, spouses, and heads of families [15]. In this regard, unified transdiagnostic therapy can be helpful for these people. Indeed, this approach's flexibility for using and integrating specific treatment interventions is one of its advantages. Based on a transdiagnostic point of view, it is understandable that people may be influenced by negative thoughts and emotions and some physiological arousals after traumatic events. Efforts to prevent remembering memories, suppression of thoughts and emotions, and other inconsistent strategies for regulating problematic emotions have a role in PTSD development rather than consistent responsiveness [8]. Thus, adaptive emotion-regulating skills using an integrated protocol can counteract the avoidance and other emotion-oriented behaviors that play a role in reinforcing and maintaining PTSD symptoms.
Based on the results, it is suggested to investigate such interventions on other psychological issues related to veterans, such as marital quality, using different methods such as a follow-up test. As a result, such interventions are recommended for people who have difficulty cognitively regulating emotion, experiential avoidance, and the diagnostic symptoms of PTSD. This treatment helps clients establish avoidance and develop adaptive emotion regulation skills coping with unpleasant emotions. Considering that unified transdiagnostic therapy targets transdiagnostic factors, it significantly affects veterans' recovery process and adaptation. Therefore, this treatment will effectively improve cognitive emotion regulation, experiential avoidance and reduce the diagnostic symptoms of PTSD.
Conclusion
Transdiagnostic therapy is effective on cognitive regulation of emotion, experimental avoidance, and reduction of PTSD symptoms in veterans with 50-70% disability in Mashhad city.
Acknowledgment: We appreciate all veterans who participated in the present study.
Ethical Permissions: The present research has been approved in terms of content and ethics by the Postgraduate Education Council of the Faculty of Psychology of Semnan University on 11/20/98, No. 34801.
Conflicts of Interests: None declared by the authors.
Authors' Contribution: Ghiyasi Noei A (First Author), Introduction Writer/Discussion Writer (34%); Sabahi P (Second Author), Methodologist/Statistical Analyst (33%); Rafieinia P (Third Author), Assistant Researcher (33%)
Funding/Support: The present study was extracted from the master thesis by Ali Ghiyasi Noei in clinical psychology and was conducted with the financial support of Semnan University.
References
1. Williams JL, Hardt MM, Henschel AV, Eddinger JR. Experiential avoidance moderates the association between motivational sensitivity and prolonged grief but not posttraumatic stress symptoms. Psychiatry Res. 2019;273:336-42. [Link] [DOI:10.1016/j.psychres.2019.01.020] [PMID] [PMCID]
2. Basharpoor S, Shafiei M, Daneshvar S. The comparison of experimental avoidance, mindfulness and rumination in trauma-exposed individuals with and without posttraumatic stress disorder (PTSD) in an Iranian sample. Arch Psychiatric Nurs. 2015;29(5):279-83. [Link] [DOI:10.1016/j.apnu.2015.05.004] [PMID]
3. Wharton E, Edwards KS, Juhasz K, Walser RD. Acceptance-based interventions in the treatment of PTSD: Group and individual pilot data using Acceptance and Commitment Therapy. J Context Behav Sci. 2019;14:55-64. [Link] [DOI:10.1016/j.jcbs.2019.09.006]
4. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5). New York: American Psychiatric Pub; 2013. [Link] [DOI:10.1176/appi.books.9780890425596]
5. Huang Q, Zhang Q, An Y Xu W. The relationship between dispositional mindfulness and PTSD/PTG among firefighters: the mediating role of emotion regulation. Personal Individ Differ. 2019;151:109492. [Link] [DOI:10.1016/j.paid.2019.07.002]
6. Diener E, Ryan K. Subjective well-being: A general overview. South Afr J Psychol. 2009;39(4):391-406. [Link] [DOI:10.1177/008124630903900402]
7. Garnefski N, Kraaij V. Cognitive emotion regulation questionnaire-development of a short 18-item version (CERQ-short). Personal Individ Differ. 2006;41(6):1045-53. [Link] [DOI:10.1016/j.paid.2006.04.010]
8. Gros DF, Allan NP. A randomized controlled trial comparing Transdiagnostic Behavior Therapy (TBT) and behavioral activation in veterans with affective disorders. Psychiatry Res. 2019;281:112541. [Link] [DOI:10.1016/j.psychres.2019.112541] [PMID]
9. McLean CP, Zang Y, Gallagher T, Suzuki N, Yarvis JS, Litz BT, et al. Trauma-related cognitions and cognitive emotion regulation as mediators of PTSD change among treatment-seeking active-duty military personnel with PTSD. Behav Ther. 2019;50(6):1053-62. [Link] [DOI:10.1016/j.beth.2019.03.006] [PMID]
10. Kelly MM, DeBeer BB, Meyer EC, Kimbrel NA, Gulliver SB, Morissette SB. Experiential avoidance as a mediator of the association between posttraumatic stress disorder symptoms and social support: a longitudinal analysis. Psychol Trauma. 2019;11(3):353-9. [Link] [DOI:10.1037/tra0000375] [PMID] [PMCID]
11. Leahy RL, Tirch D, Napolitano LA. Emotion regulation in psychotherapy: a practitioner's guide. New York: Guilford Press; 2011. [Link]
12. Seligowski AV, Rogers AP, Orcutt HK. Relations among emotion regulation and DSM-5 symptom clusters of PTSD. Personal Individ Differ. 2016;92:104-8. [Link] [DOI:10.1016/j.paid.2015.12.032]
13. Raines EM, Rogers AH, Bakhshaie J, Viana AG, Lemaire C, Garza M, et al. Mindful attention moderating the effect of experiential avoidance in terms of mental health among Latinos in a federally qualified health center. Psychiatry Res. 2018;270:574-80. [Link] [DOI:10.1016/j.psychres.2018.10.036] [PMID]
14. Difede J, Rothbaum BO, Rizzo AA, Wyka K, Spielman L, Jovanovic T, et al. Enhanced exposure therapy for combat-related Posttraumatic Stress Disorder (PTSD): study protocol for a randomized controlled trial. Contemp Clin Trials. 2019;87:105857. [Link] [DOI:10.1016/j.cct.2019.105857] [PMID]
15. Bourassa K J, Smolenski DJ, Edwards-Stewart A, Campbell SB, Reger GM, Norr AM. The impact of prolonged exposure therapy on social support and PTSD symptoms. J Affect Disord. 2020;260:410-7. [Link] [DOI:10.1016/j.jad.2019.09.036] [PMID] [PMCID]
16. Ellard KK, Fairholme CP, Boisseau CL, Farchione TJ, Barlow DH. Unified protocol for the transdiagnostic treatment of emotional disorders: Protocol development and initial outcome data. Cognit Behav Pract. 2010;17(1):88-101. [Link] [DOI:10.1016/j.cbpra.2009.06.002] [PMID] [PMCID]
17. Wilamowska ZA, Thompson‐Hollands J, Fairholme CP, Ellard KK, Farchione TJ, Barlow DH. Conceptual background, development, and preliminary data from the unified protocol for transdiagnostic treatment of emotional disorders. Depress Anxiety. 2010;27(10):882-90. [Link] [DOI:10.1002/da.20735] [PMID]
18. García-Escalera J, Valiente RM, Sandín B, Ehrenreich-May J, Prieto A, Chorot P. The unified protocol for transdiagnostic treatment of emotional disorders in adolescents (UP-A) adapted as a school-based anxiety and depression prevention program: an initial cluster randomized wait-list-controlled trial. Behav ther. 2020;51(3):461-73. [Link] [DOI:10.1016/j.beth.2019.08.003] [PMID]
19. Sakiris N, Berle D. A systematic review and meta-analysis of the unified protocol as a transdiagnostic emotion regulation based intervention. Clin Psychol Rev. 2019;72:101751. [Link] [DOI:10.1016/j.cpr.2019.101751] [PMID]
20. Hasanpoor P, Aghausefi A, Zamir O, Alipour A. The effectiveness of transdiagnostic treatment on experiential avoidance and cognitive emotion regulation in patients with obsessive-compulsive disorder and its comparison with exposure and prevention response therapy. J Clin Psychol. 2019;11(3):25-38 [Persian] [Link]
21. Fdaei M, Ghanbari Hashem Abadi B, Kimiaee S. The efficacy of integrated meta-diagnosis therapy on their differentiation and the difficulty of regulating excitement in patients with anxiety syndrome. Med J Mashhad Univ Med Sci. 2019;61 suppl 1:1-11. [Persian] [Link]
22. Osmani H, Shokri L. Effectiveness of unified trans-diagnostic treatment on emotion' s cognitive regulation and cognitive empathy of students with externalized behavior disorder. Empower Except Child. 2019;10(1):125-36. [Persian] [Link]
23. Garnefski N, Legerstee J, Kraaij VV, Van Den Kommer T, Teerds J. Cognitive coping strategies and symptoms of depression and anxiety: a comparison between adolescents and adults. J Adolesc. 2002;25(6):603-11. [Link] [DOI:10.1006/jado.2002.0507] [PMID]
24. Samani S, Joukar B. A study on the reliability and of the short form of the depression, anxiety, stress scale (DASS-21). J Soc Sci Human Shiraz Univ. 2007;26(3):65-76. [Persian] [Link]
25. Issazadegan A, Fathabadi J. The role of cognitive emotion regulation strategies and general health in alexithymia. Develop Psychol. 2012;8:257-67. [Persian] [Link]
26. Gámez W, Chmielewski M, Kotov R, Ruggero C, Watson D. Development of a measure of experiential avoidance: the multidimensional experiential avoidance questionnaire. Psychol Assess. 2011;23(3):692-713. [Link] [DOI:10.1037/a0023242] [PMID]
27. Weathers F, Litz B, Keane T, Palmieri T, Marx BP, Schnurr P. The PTSD checklist for DSM-5 (PCL-5). Chicago: International Society for Traumatic Stress Studies; 2013. [Link]
28. Talebigi F. The effectiveness of acceptance and commitment-based therapy on reducing experience avoidance in veterans with impact stress disorder in Kerman [dissertation]. Tehran: Allameh Tabatabai University; 2015. [Persian] [Link]
29. Barlow DH, Farchione TJ, Fairholme CP, Ellard KK, Boisseau CL, Allen LB, et al. Unified protocol for transdiagnostic treatment of emotional disorders: therapist guide. Oxford: Oxford University Press; 2010. [Link] [DOI:10.1093/med:psych/9780199772667.001.0001]
30. Harvey A, Watkins E, Mansell W, Shafran R. Cognitive behavioral processes across psychological disorders: a transdiagnostic approach to research and treatment. Oxford: Oxford University Press; 2004. [Link] [DOI:10.1093/med:psych/9780198528883.001.0001]
31. Bullis JR, Fortune MR, Farchione TJ, Barlow DH. A preliminary investigation of the long-term outcome of the unified protocol for transdiagnostic treatment of emotional disorders. Compr Psychiatry. 2014;55(8):1920-7. [Link] [DOI:10.1016/j.comppsych.2014.07.016] [PMID] [PMCID]
32. Banducci AN, Bujarski SJ, Bonn-Miller MO, Patel A, Connolly KM. The impact of intolerance of emotional distress and uncertainty on veterans with co-occurring PTSD and substance use disorders. J Anxiety Disord. 2016;41:73-81. [Link] [DOI:10.1016/j.janxdis.2016.03.003] [PMID]