
JMERC
Owner
Janbazan Medical and Engineering Research Center (JMERC) is the owner of IJWPH.

0.3
Cite Score
SJR: 0.114 / SNIP: 0.090
Volume 13, Issue 1 (2021)
Iran J War Public Health 2021, 13(1): 31-40 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2021/01/9 | Accepted: 2021/07/12 | Published: 2021/09/26
Received: 2021/01/9 | Accepted: 2021/07/12 | Published: 2021/09/26
How to cite this article
Yousefi N, Tofangchiha S, Rahnejat A. Body Image and Shame with Adult Attachment Mediation in War-Related Amputation: A Structural Model. Iran J War Public Health 2021; 13 (1) :31-40
URL: http://ijwph.ir/article-1-948-en.html
URL: http://ijwph.ir/article-1-948-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Department of Clinical Psychology, Medical Faculty, Aja University of Medical Sciences (AUMS), Tehran, Iran
2- Department of Internal Medicine, Medical Faculty, Aja University of Medical Sciences (AUMS), Tehran, Iran , Stofangchiha@yahoo.com
2- Department of Internal Medicine, Medical Faculty, Aja University of Medical Sciences (AUMS), Tehran, Iran , Stofangchiha@yahoo.com
Full-Text (HTML) (1064 Views)
Introduction
War imposes irreparable adverse effects with whatever character and purpose it occurs and can have both positive and negative effects. The negative effects of war are more tangible and overshadow its positive effects. The first negative but tangible and direct impacts of war appear in human and civil dimensions [1]. Most of the problems and consequences of war appear after the flames of war have subsided. The damage caused by the eight-year Iran-Iraq war is estimated at 80 billion dollars, according to statistics provided by the Economic Commission for the Estimation of War Damage. This figure is equivalent to seven years of total foreign exchange earnings from the sale of oil and gas in the country or equivalent to 30 years of foreign exchange earnings earned from non-oil exports. It is noteworthy that this figure covers the period from the beginning of the war to the end of 1983 and does not include the losses that occurred during the following years, thus, billions of dollars of direct and indirect economic damage to Iran [2].
However, it is worth noting that regardless of the economic damage and consequences, war has irreparable consequences in the human dimension, so that the statistics of diseases and mental disorders are not equal to the extent of the war in any period of the social life of the people of a society. The eight-year war against Iraq has left about half a million veterans for Iran [3]. Even though three decades have passed since the end of the war, the veterans and their families are no longer expected to have problems in their personal and social lives; the evidence shows that survivors still feel the war-related suffering and consequences. In this regard, amputation or loss of a limb or part of it is one of the common events of recent decades. Annually, due to factors such as war and disease, there are about 500 to 200 million amputations worldwide, of which in the United States, for example, about 1.7 million people live with amputations [4]. Sarvestani & Azam [5], in their study entitled "Amputation: a ten-year survey," reported that the average age of Iranian amputees was 39 years, of which 79% were men and 20% were women. This statistic means that labor forces and the young population make up a large part of these people, and it is necessary to solve their problems. As is clear, the Department of Veterans Affairs has focused on improving the care of veteran amputees worldwide over the past decade [6]. This is important because the amputation process poses a significant physical and psychological challenge for individuals. Regardless of its causes, amputation can undoubtedly be a very stressful experience that requires psychological and physical adjustment over a wide period. The results of review studies suggest that veteran amputees experience symptoms of depression, anxiety (especially social anxiety) and body image disturbance [7]. Physically, amputation can cause pain, movement and balance problems (especially in people with lower-limb amputations) and problems with self-care skills. However, finding a solution to eliminating the adverse psychological effects of amputation is as important as the physical rehabilitation of these people [8].
With regard to the psychological dimension, amputation causes a gap in three dimensions: functional, emotional and body image [9]. The body image dimension should be paid more attention to because body image plays a significant role in social and interpersonal communication. Appearance changes caused by trauma or illness can completely change a person's body image and take them away from their ideal image who try to hide from others [10]. Body image is defined as a person's thoughts, feelings, and behaviors about physical appearance and function. People who experience amputation-induced physical deformity are vulnerable to physical concerns and social stigma [8] and may limit their social interactions simply because they feel insecure in such situations, lack knowledge of proper behavior, being afraid of how to be treated or try to avoid unwanted situations [11]; Thus, body image is related with psychological adjustment, and changes in a person's appearance can trigger a set of psychological, perceptual, and emotional reactions [9]. For some people, body image-related concerns may precede adaptation processes and play a secondary role for others. However, the development of an integrated body image after amputation is a key part of the rehabilitation process in most people, and this shows that it is very important to pay attention to the issue of body image in amputees. Considering the complex effects of amputation on appearance and bodily function, body image should be considered the main core in understanding the adaptation concept in these people [8]. Various studies have investigated the effect of body image on the psychological dimensions of amputees [7-12]. They have shown that it is very important to investigate body image-related concerns among amputees and their relationship with psychological adaptation to alteration of body image [13, 14].
In this regard, research shows that body image-related concerns, including body dissatisfaction, are associated with symptoms of many mental disorders and distresses, including general negative impact, depression, anxiety, low self-esteem, eating disorders, muscle deformity, sexual dysfunction, and poor quality of life [15]. Many studies [16-21] also show that body image can be a source of shame. Shame attacks the core of one's identity and is associated with feelings of diminution, worthlessness, and inability [22], which is seen in veteran amputees due to some inability to do certain affairs independently. It should be noted that such shame can affect self-esteem, sociability and self-care, or seeking the care of military forces and veteran amputees [17]. The focus is on the "self" as a whole concerning shame. Shame arises from the difference between self and self-ideal. In this case, shame is defined as an emotion-based on depressing feelings such as despair, stupidity, and desire to avoid being with others for fear of rejection [23]. Arditte et al. [24] found that people prone to shame are more likely to experience psychological and interpersonal problems. According to the clinical psychology literature, the role of shame has been identified in all major categories of disorder-related injury [25]. It is associated with many psychological problems, including obsessive-compulsive disorder [26], substance use disorder [27], and eating disorders [28], interpersonal sensitivity, low self-esteem, emotion regulation, psychological well-being and susceptibility to aggression [29]. Shame is usually accompanied by painful emotion, often with perceptions of one's characteristics (e.g., body shape, size with appearance), personality traits (boredom) or behaviors that do not seem interesting to others (e.g., cheating, stealing), which in turn lead to rejection or some form of social decline. There are two types of shame that is external and internal. External shame relates to thoughts and feelings of how one looks in the minds of others. In this shame, the focus is on the views of others. Internal shame is manifested by the growth of self-awareness and how one manifests oneself to others [30]. The focus of this shame is on feelings and self- self-devaluation as an incompetent person. One of the important components of internal shame is self-evaluation and self-criticism. It seems that shame can easily make people busy thinking about self-critical styles and increase vulnerability in the face of a wide range of problems [31]. Previous researches have investigated the relationship between shame with the problems of veterans. For example, a study [32] on the differential relationship between guilt and shame about post-traumatic stress disorder among veterans, research [33] on the traumatic experiences of combat veterans and its relationship with feelings of shame and guilt, and research [34] on shame as a mediator between the symptoms of post-traumatic stress disorder and the suicide ideation among veterans. In the meantime, there was no study on the relationship between the body image and shame mediated by adult attachment, which is regarded as a concern of the present study because one of the causes of shame can be the physical conditions and physical disability of individuals [21]. On the other hand, in addition to the direct relationship between the two variables of shame and amputation, these components are closely related to attachment styles, as mentioned in the latest research [35].
According to the attachment theory, failure in the secure attachment process is the source of many problems and diseases [36]. Bowlby first introduced attachment theory in 1982 to explain the strong emotional bonds between infants and their mothers (or other primary caregivers). These bonds are formed by the quality of care provided by the parents or the parent symbol. Secure attachment is characterized by a sense of self-worth and trust in others, and conversely, insecure attachment is defined as a lack of trust in relationships, and a sense of worthlessness in receiving love from important others, all influenced by adult relationships. Attachment patterns formed during childhood are believed to be stable throughout life, although experiences of different relationships (positive or negative) during adulthood may later change these representations [37]. Adult attachment style is regulated by the attachment system. Attachment is an innate behavior that aims to protect the individual and maintain survival [38]. At birth, the child seeks to explore the unknown world, where attachment serves as a support base in discovering the extent of the universe and helping the child to discover the unknown [39]. Attachment is an important psychological trait in which the weaker and less able person (child) needs the support of a more competent and powerful person (important other) in times of stress, even during adulthood. One of Bowlby's basic attachment hypotheses was that the attachment-behavioral system evolved to play an important role in protecting infants from environmental hazards through the physical proximity of primary caregivers to the child [40]. Bowlby has divided attachment into secure attachment, ambivalent-insecure attachment, and avoidant-insecure attachment [37]. Secure attachment leads to improved performance, success, and satisfaction. A person with secure attachment is less concerned about being evaluated by others [39].
On the other hand, people with insecure attachments have less understanding of others, do not trust others, are upset by closeness and intimacy, and have fewer cognitive-emotional deficits than people with secure attachments. People with an insecure attachment seems to be very dependent due to fear of separation (hyperactivity of the attachment system), their relationship is inflexible, and they are almost cared for forcefully [39]. Models of internalization of attachment styles are dynamic, and in situations where a person experiences a crisis, attachment styles may change according to new situations [41]. Although the secure attachment model shows relative stability, studies have been conducted on various accidents and injuries that can change the attachment style throughout life [39].
Considering the preceding, it can be said that amputation has an undeniable effect on mental status and family and social relationships because physical disability and psychosocial adaptation affect mental health and such people are more socially isolated than normal people [8]. Life after amputation is associated with many problems in these people. These people suffer from psychosocial problems such as depression, feelings of hopelessness, low self-confidence, fatigue, anxiety, frustration, poor social performance, and body image anxiety due to non-adaptation to new situations [7-12]. Hence, it is sufficient to think about the physical issue among veteran amputees, but these people can face many psychological conflicts. Stress, anxiety, shame, and body dysmorphic disorder among veteran amputees are important factors in using ineffective coping strategies that can positively affect problem-solving and rational acceptance of the situation for these patients. This can lead to an irrational cycle that aggravates their mental disorders and also slows down their recovery. Therefore, it seems that therapists and psychologists need to pay attention to the physical treatment of this disease and their psychological disorders to treat veteran amputees. Therefore, such studies are very necessary.
Veterans constitute an important part of the military community who have been harmed while defending the country's ideals. Medical and psychological care for these people and improving their quality of life can lead us to have a plan for veteran amputees in the future. There was no research on the structural model of shame-based body image mediated by adult attachment among veteran amputees in domestic and foreign scientific databases. Therefore, the present study aimed to provide a model by examining body image and shame mediated by adult attachment among veteran amputees to provide a plan for military psychologists to have a psychological model for the military in an accident and amputation.
Instrument & Methods
This Descriptive research was conducted on male veterans who underwent one-sided major amputation (above ankle or wrist) in Tehran, Iran, in 2020. According to the statistics of the Foundation of Martyrs and Veterans, the number of impaired veterans in Tehran is estimated at approximately 17,000, of which 195 were selected as sample. Convenience sampling was applied to select the samples. Amputees were identified through various channels (including Shahed schools, Municipality of Tehran). The questioners took the questionnaires to any place selected by the participants (home, workplace or any other places). Sampling continued from January 2020 to June 2020. It should be noted that almost all of the required information was collected before the covid-19 pandemic, and after the pandemic in Iran, due to the sensitivity of the study population, sampling was performed according to strict criteria. In cases where it was not possible to access the veterans in person, questionnaires were sent to them through social networks, the number of which was 44. In order to determine the sample size, considering 12 items for each variable in multiple regression analysis and modeling is an acceptable rule. The number of main variables and their dimensions in the research was 15. Accordingly, 12 amputees were considered for each variable. Therefore, the final number of sample size was 180 amputees, which was considered 200 to compensate for possible loss. The criteria for inclusion were less than 70 years old, a minimum of a Diploma, no cognitive or intelligence problems, and not receiving psychological intervention during the study. The cases that were illegible, distorted or incomplete were excluded.
Four questionnaires were used.
-Demographic questionnaire includes age, level of education, marital status, number of children, employment status (retired or employed), history of physical illness, history of mental illness (if any, type of illness).
-The Attachment style questionnaire was developed by Collins & Readin [42]. The questions were scored based on a 5-point Likert scale (using scores ranging from 1: Does not match my characteristics at all to 5: perfectly matches my characteristics). The questionnaire consists of three subscales: Anxious style: It corresponds to the ambivalent attachment style and measures the fear of having a relationship. Intimacy style corresponds to a secure attachment style and measures comfort concerning intimacy and emotional closeness. Avoidant style: It includes the amount of trust that subjects place in others and rely on them. Questions 1, 8, 9, 10, 14 and 17 measure secure attachment; questions 3, 4, 7, 15, 16, and 18 measure avoidant attachment; and questions 2, 5, 6, 11, 12, and 13 measure anxious attachment [42]. In a pioneering study on 105 girls and boys in Tehran by Pakdaman [43], this questionnaire's test-retest reliability and validity were 0.97 and 0.56, respectively. In research [44], the reliability of the whole questionnaire and secure, avoidant, and ambivalent/anxious subscales was obtained at 0.82, 0.89, 0.81, and 0.77 by measuring Cronbach's alpha, respectively. In the present study, Cronbach's alpha coefficient of secure, avoidant, and ambivalent/anxious subscales was obtained 0.76, 0.81, and 0.79, respectively.
-Multidimensional Body–Self Relations Questionnaire (MBSRQ) consists of 69 items designed by Brown et al. [45]. It assesses a person's attitude about different dimensions of body image structure. This questionnaire can be used by people 15 years and older and is not suitable for assessing children. The questions of this questionnaire are scored based on the 5-point Likert scale (1: Strongly disagree to 5: Strongly agree) for each item. It should be noted that for questions to be reverse scored, this scoring is (completely agree=1 to disagree=5). The questions which are to be reverse scored are as follows: 47, 37, 38, 28, 45, 30, 17, 43, 34, 25, 25, 16, 15, 6, 33, 49, 40, 32, 23, 48, and 42. Higher scores indicate better body image perception. The subscales of this questionnaire include: Appearance evaluation (48, 42, 39, 30, 21, 11, 5), appearance orientation (50, 49, 41, 40, 32, 31, 23, 22, 13, 12, 2, 1), fitness evaluation (51, 33, 24), fitness orientation (53, 44, 43, 35, 34, 26, 25, 16, 15, 14, 6, 4, 3), health evaluation (54, 45, 30, 27, 17, 7), health orientation (52, 38, 29, 28, 19, 18, 9, 8) illness orientation (56, 55, 47, 46, 37), body areas satisfaction (69-61), subjective weight (60, 59), weight preoccupation (58, 57, 28, 10). The validity of the main parts of the questionnaire was assessed by Brown et al. [45]. The questionnaire validity was estimated at 0.79 using content validity. Also, the reliability of the whole instrument was reported to be 0.81 [45]. In a study by Zarshenas et al. [46], the reliability of the subscales of appearance awareness, appearance evaluation, weight preoccupation, body areas satisfaction, and subjective evaluation was reported 0.87, 0.85, 0.82, 0.79, and 0.75, respectively. The reliability of this questionnaire the subscales of appearance evaluation, appearance orientation, fitness evaluation, fitness orientation, health evaluation, health orientation, illness orientation, physical satisfaction, subjective weight, weight preoccupation, and total score of the questionnaire was obtained α=0.74, α=0.79, α=0.85, α=0.81, α=0.74, α=0.86, α=0.81, α=0.80, α=0.79, α=0.77, and α=0.77, respectively.
-Shame questionnaire was developed by Cook [47]. This questionnaire consists of 30 questions and two subscales of shyness with 24 items (1, 2, 3, 4, 5, 6, 7, 9, 10, 11, 12, 15, 16, 17, 18, 20, 21, 22, 23, 24, 25, 27, 28, 30) and self-esteem with 6 items (8, 13, 14, 19, 26, 29). Questions are answered based on a 5-point Likert scale (Never: 0; Always: 4). The possible score range is 0 and 120. A high score indicates worthlessness, incompetence, and feelings of inferiority, emptiness, and loneliness. However, a low score indicates high self-confidence. Cook reported the Cronbach's alpha reliability coefficient of the shyness and low self-esteem subscales as 0.94 and 0.90, respectively. This researcher stated that the content validity of this questionnaire is acceptable (CVI=0.88) [47]. In a study by Rajabi & Abbasi [48], Cronbach's alpha reliability coefficients of the Shame Questionnaire were reported 0.90 for the whole sample, 0.89 for men, and 0.91 for women. In the present study, the reliability of subscales of shyness and low self-esteem and the total score of the questionnaire was reported α=0.85, α=0.89, and α=0.87, respectively.
The study was approved by the Ethics Committee of Aja University of Medical Sciences. The questioners took the questionnaires to any place selected by the participants (home, workplace, or any other place). The purpose of this study was explained to the participants, and their consent to participate in this study was considered, and they were allowed to
leave it at any stage of the process they wanted. In a private space, they were asked to complete the questionnaires and give them to the questioners. Due to the covid-19 conditions and the ease of work of participants, the online questionnaire option was also offered to them; thus, 48 questionnaires were filled in online.
Correlational structural equation modeling -a combination of path analysis and confirmatory factor analysis- was used. Pearson correlation matrix, multiple regression, and path analysis were used to analyze inferential statistics and frequency, the mean and standard deviation for descriptive statistics, and hypothesis testing. Data were analyzed by SPSS 25 and Amos 23.
Findings
Finally 195 questionnaires were analyzed. Demographic findings showed in Table 1.
Results of body image, shame, and attachment style among veteran amputees were showed in Table 2.
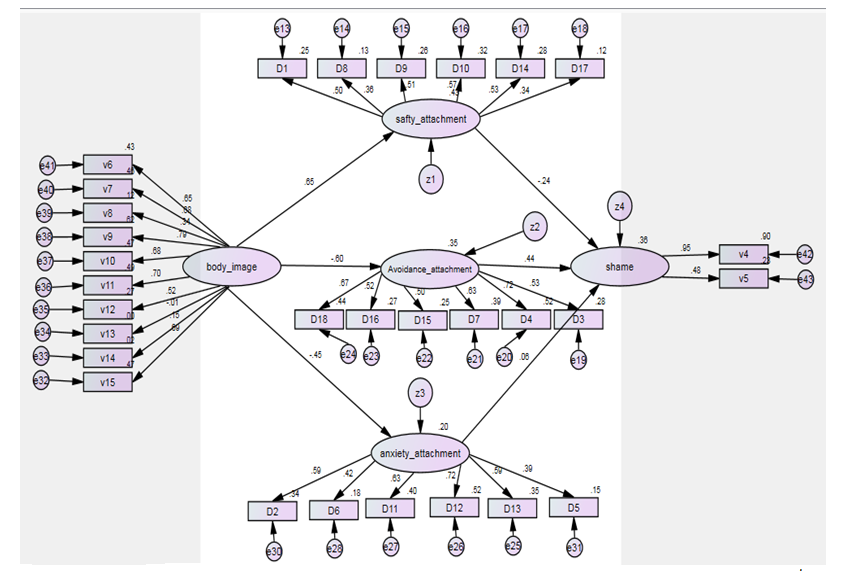
The results indicate an acceptable fit of the proposed model (Table 3). The general model proposed had a good fit. The g path coefficients were significant in all paths (p<0.05). Also, all β coefficients of shame attachment styles were significant (p<0.05). This means that the assumed direct causal paths of the general pattern were well-validated, and its indirect paths were confirmed (Figure 1).
Table 1) Demographic findings of participants in the research sample group (N=195)
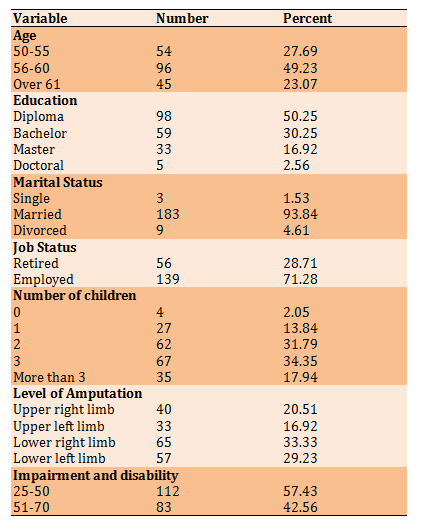
Table 2) Descriptive findings of body image, shame, and attachment style among veteran amputees

Table 3) Fit indices of the proposed model

Figure 1) The final structural pattern of shame-based model based on body image mediated by attachment styles among veteran amputees
War imposes irreparable adverse effects with whatever character and purpose it occurs and can have both positive and negative effects. The negative effects of war are more tangible and overshadow its positive effects. The first negative but tangible and direct impacts of war appear in human and civil dimensions [1]. Most of the problems and consequences of war appear after the flames of war have subsided. The damage caused by the eight-year Iran-Iraq war is estimated at 80 billion dollars, according to statistics provided by the Economic Commission for the Estimation of War Damage. This figure is equivalent to seven years of total foreign exchange earnings from the sale of oil and gas in the country or equivalent to 30 years of foreign exchange earnings earned from non-oil exports. It is noteworthy that this figure covers the period from the beginning of the war to the end of 1983 and does not include the losses that occurred during the following years, thus, billions of dollars of direct and indirect economic damage to Iran [2].
However, it is worth noting that regardless of the economic damage and consequences, war has irreparable consequences in the human dimension, so that the statistics of diseases and mental disorders are not equal to the extent of the war in any period of the social life of the people of a society. The eight-year war against Iraq has left about half a million veterans for Iran [3]. Even though three decades have passed since the end of the war, the veterans and their families are no longer expected to have problems in their personal and social lives; the evidence shows that survivors still feel the war-related suffering and consequences. In this regard, amputation or loss of a limb or part of it is one of the common events of recent decades. Annually, due to factors such as war and disease, there are about 500 to 200 million amputations worldwide, of which in the United States, for example, about 1.7 million people live with amputations [4]. Sarvestani & Azam [5], in their study entitled "Amputation: a ten-year survey," reported that the average age of Iranian amputees was 39 years, of which 79% were men and 20% were women. This statistic means that labor forces and the young population make up a large part of these people, and it is necessary to solve their problems. As is clear, the Department of Veterans Affairs has focused on improving the care of veteran amputees worldwide over the past decade [6]. This is important because the amputation process poses a significant physical and psychological challenge for individuals. Regardless of its causes, amputation can undoubtedly be a very stressful experience that requires psychological and physical adjustment over a wide period. The results of review studies suggest that veteran amputees experience symptoms of depression, anxiety (especially social anxiety) and body image disturbance [7]. Physically, amputation can cause pain, movement and balance problems (especially in people with lower-limb amputations) and problems with self-care skills. However, finding a solution to eliminating the adverse psychological effects of amputation is as important as the physical rehabilitation of these people [8].
With regard to the psychological dimension, amputation causes a gap in three dimensions: functional, emotional and body image [9]. The body image dimension should be paid more attention to because body image plays a significant role in social and interpersonal communication. Appearance changes caused by trauma or illness can completely change a person's body image and take them away from their ideal image who try to hide from others [10]. Body image is defined as a person's thoughts, feelings, and behaviors about physical appearance and function. People who experience amputation-induced physical deformity are vulnerable to physical concerns and social stigma [8] and may limit their social interactions simply because they feel insecure in such situations, lack knowledge of proper behavior, being afraid of how to be treated or try to avoid unwanted situations [11]; Thus, body image is related with psychological adjustment, and changes in a person's appearance can trigger a set of psychological, perceptual, and emotional reactions [9]. For some people, body image-related concerns may precede adaptation processes and play a secondary role for others. However, the development of an integrated body image after amputation is a key part of the rehabilitation process in most people, and this shows that it is very important to pay attention to the issue of body image in amputees. Considering the complex effects of amputation on appearance and bodily function, body image should be considered the main core in understanding the adaptation concept in these people [8]. Various studies have investigated the effect of body image on the psychological dimensions of amputees [7-12]. They have shown that it is very important to investigate body image-related concerns among amputees and their relationship with psychological adaptation to alteration of body image [13, 14].
In this regard, research shows that body image-related concerns, including body dissatisfaction, are associated with symptoms of many mental disorders and distresses, including general negative impact, depression, anxiety, low self-esteem, eating disorders, muscle deformity, sexual dysfunction, and poor quality of life [15]. Many studies [16-21] also show that body image can be a source of shame. Shame attacks the core of one's identity and is associated with feelings of diminution, worthlessness, and inability [22], which is seen in veteran amputees due to some inability to do certain affairs independently. It should be noted that such shame can affect self-esteem, sociability and self-care, or seeking the care of military forces and veteran amputees [17]. The focus is on the "self" as a whole concerning shame. Shame arises from the difference between self and self-ideal. In this case, shame is defined as an emotion-based on depressing feelings such as despair, stupidity, and desire to avoid being with others for fear of rejection [23]. Arditte et al. [24] found that people prone to shame are more likely to experience psychological and interpersonal problems. According to the clinical psychology literature, the role of shame has been identified in all major categories of disorder-related injury [25]. It is associated with many psychological problems, including obsessive-compulsive disorder [26], substance use disorder [27], and eating disorders [28], interpersonal sensitivity, low self-esteem, emotion regulation, psychological well-being and susceptibility to aggression [29]. Shame is usually accompanied by painful emotion, often with perceptions of one's characteristics (e.g., body shape, size with appearance), personality traits (boredom) or behaviors that do not seem interesting to others (e.g., cheating, stealing), which in turn lead to rejection or some form of social decline. There are two types of shame that is external and internal. External shame relates to thoughts and feelings of how one looks in the minds of others. In this shame, the focus is on the views of others. Internal shame is manifested by the growth of self-awareness and how one manifests oneself to others [30]. The focus of this shame is on feelings and self- self-devaluation as an incompetent person. One of the important components of internal shame is self-evaluation and self-criticism. It seems that shame can easily make people busy thinking about self-critical styles and increase vulnerability in the face of a wide range of problems [31]. Previous researches have investigated the relationship between shame with the problems of veterans. For example, a study [32] on the differential relationship between guilt and shame about post-traumatic stress disorder among veterans, research [33] on the traumatic experiences of combat veterans and its relationship with feelings of shame and guilt, and research [34] on shame as a mediator between the symptoms of post-traumatic stress disorder and the suicide ideation among veterans. In the meantime, there was no study on the relationship between the body image and shame mediated by adult attachment, which is regarded as a concern of the present study because one of the causes of shame can be the physical conditions and physical disability of individuals [21]. On the other hand, in addition to the direct relationship between the two variables of shame and amputation, these components are closely related to attachment styles, as mentioned in the latest research [35].
According to the attachment theory, failure in the secure attachment process is the source of many problems and diseases [36]. Bowlby first introduced attachment theory in 1982 to explain the strong emotional bonds between infants and their mothers (or other primary caregivers). These bonds are formed by the quality of care provided by the parents or the parent symbol. Secure attachment is characterized by a sense of self-worth and trust in others, and conversely, insecure attachment is defined as a lack of trust in relationships, and a sense of worthlessness in receiving love from important others, all influenced by adult relationships. Attachment patterns formed during childhood are believed to be stable throughout life, although experiences of different relationships (positive or negative) during adulthood may later change these representations [37]. Adult attachment style is regulated by the attachment system. Attachment is an innate behavior that aims to protect the individual and maintain survival [38]. At birth, the child seeks to explore the unknown world, where attachment serves as a support base in discovering the extent of the universe and helping the child to discover the unknown [39]. Attachment is an important psychological trait in which the weaker and less able person (child) needs the support of a more competent and powerful person (important other) in times of stress, even during adulthood. One of Bowlby's basic attachment hypotheses was that the attachment-behavioral system evolved to play an important role in protecting infants from environmental hazards through the physical proximity of primary caregivers to the child [40]. Bowlby has divided attachment into secure attachment, ambivalent-insecure attachment, and avoidant-insecure attachment [37]. Secure attachment leads to improved performance, success, and satisfaction. A person with secure attachment is less concerned about being evaluated by others [39].
On the other hand, people with insecure attachments have less understanding of others, do not trust others, are upset by closeness and intimacy, and have fewer cognitive-emotional deficits than people with secure attachments. People with an insecure attachment seems to be very dependent due to fear of separation (hyperactivity of the attachment system), their relationship is inflexible, and they are almost cared for forcefully [39]. Models of internalization of attachment styles are dynamic, and in situations where a person experiences a crisis, attachment styles may change according to new situations [41]. Although the secure attachment model shows relative stability, studies have been conducted on various accidents and injuries that can change the attachment style throughout life [39].
Considering the preceding, it can be said that amputation has an undeniable effect on mental status and family and social relationships because physical disability and psychosocial adaptation affect mental health and such people are more socially isolated than normal people [8]. Life after amputation is associated with many problems in these people. These people suffer from psychosocial problems such as depression, feelings of hopelessness, low self-confidence, fatigue, anxiety, frustration, poor social performance, and body image anxiety due to non-adaptation to new situations [7-12]. Hence, it is sufficient to think about the physical issue among veteran amputees, but these people can face many psychological conflicts. Stress, anxiety, shame, and body dysmorphic disorder among veteran amputees are important factors in using ineffective coping strategies that can positively affect problem-solving and rational acceptance of the situation for these patients. This can lead to an irrational cycle that aggravates their mental disorders and also slows down their recovery. Therefore, it seems that therapists and psychologists need to pay attention to the physical treatment of this disease and their psychological disorders to treat veteran amputees. Therefore, such studies are very necessary.
Veterans constitute an important part of the military community who have been harmed while defending the country's ideals. Medical and psychological care for these people and improving their quality of life can lead us to have a plan for veteran amputees in the future. There was no research on the structural model of shame-based body image mediated by adult attachment among veteran amputees in domestic and foreign scientific databases. Therefore, the present study aimed to provide a model by examining body image and shame mediated by adult attachment among veteran amputees to provide a plan for military psychologists to have a psychological model for the military in an accident and amputation.
Instrument & Methods
This Descriptive research was conducted on male veterans who underwent one-sided major amputation (above ankle or wrist) in Tehran, Iran, in 2020. According to the statistics of the Foundation of Martyrs and Veterans, the number of impaired veterans in Tehran is estimated at approximately 17,000, of which 195 were selected as sample. Convenience sampling was applied to select the samples. Amputees were identified through various channels (including Shahed schools, Municipality of Tehran). The questioners took the questionnaires to any place selected by the participants (home, workplace or any other places). Sampling continued from January 2020 to June 2020. It should be noted that almost all of the required information was collected before the covid-19 pandemic, and after the pandemic in Iran, due to the sensitivity of the study population, sampling was performed according to strict criteria. In cases where it was not possible to access the veterans in person, questionnaires were sent to them through social networks, the number of which was 44. In order to determine the sample size, considering 12 items for each variable in multiple regression analysis and modeling is an acceptable rule. The number of main variables and their dimensions in the research was 15. Accordingly, 12 amputees were considered for each variable. Therefore, the final number of sample size was 180 amputees, which was considered 200 to compensate for possible loss. The criteria for inclusion were less than 70 years old, a minimum of a Diploma, no cognitive or intelligence problems, and not receiving psychological intervention during the study. The cases that were illegible, distorted or incomplete were excluded.
Four questionnaires were used.
-Demographic questionnaire includes age, level of education, marital status, number of children, employment status (retired or employed), history of physical illness, history of mental illness (if any, type of illness).
-The Attachment style questionnaire was developed by Collins & Readin [42]. The questions were scored based on a 5-point Likert scale (using scores ranging from 1: Does not match my characteristics at all to 5: perfectly matches my characteristics). The questionnaire consists of three subscales: Anxious style: It corresponds to the ambivalent attachment style and measures the fear of having a relationship. Intimacy style corresponds to a secure attachment style and measures comfort concerning intimacy and emotional closeness. Avoidant style: It includes the amount of trust that subjects place in others and rely on them. Questions 1, 8, 9, 10, 14 and 17 measure secure attachment; questions 3, 4, 7, 15, 16, and 18 measure avoidant attachment; and questions 2, 5, 6, 11, 12, and 13 measure anxious attachment [42]. In a pioneering study on 105 girls and boys in Tehran by Pakdaman [43], this questionnaire's test-retest reliability and validity were 0.97 and 0.56, respectively. In research [44], the reliability of the whole questionnaire and secure, avoidant, and ambivalent/anxious subscales was obtained at 0.82, 0.89, 0.81, and 0.77 by measuring Cronbach's alpha, respectively. In the present study, Cronbach's alpha coefficient of secure, avoidant, and ambivalent/anxious subscales was obtained 0.76, 0.81, and 0.79, respectively.
-Multidimensional Body–Self Relations Questionnaire (MBSRQ) consists of 69 items designed by Brown et al. [45]. It assesses a person's attitude about different dimensions of body image structure. This questionnaire can be used by people 15 years and older and is not suitable for assessing children. The questions of this questionnaire are scored based on the 5-point Likert scale (1: Strongly disagree to 5: Strongly agree) for each item. It should be noted that for questions to be reverse scored, this scoring is (completely agree=1 to disagree=5). The questions which are to be reverse scored are as follows: 47, 37, 38, 28, 45, 30, 17, 43, 34, 25, 25, 16, 15, 6, 33, 49, 40, 32, 23, 48, and 42. Higher scores indicate better body image perception. The subscales of this questionnaire include: Appearance evaluation (48, 42, 39, 30, 21, 11, 5), appearance orientation (50, 49, 41, 40, 32, 31, 23, 22, 13, 12, 2, 1), fitness evaluation (51, 33, 24), fitness orientation (53, 44, 43, 35, 34, 26, 25, 16, 15, 14, 6, 4, 3), health evaluation (54, 45, 30, 27, 17, 7), health orientation (52, 38, 29, 28, 19, 18, 9, 8) illness orientation (56, 55, 47, 46, 37), body areas satisfaction (69-61), subjective weight (60, 59), weight preoccupation (58, 57, 28, 10). The validity of the main parts of the questionnaire was assessed by Brown et al. [45]. The questionnaire validity was estimated at 0.79 using content validity. Also, the reliability of the whole instrument was reported to be 0.81 [45]. In a study by Zarshenas et al. [46], the reliability of the subscales of appearance awareness, appearance evaluation, weight preoccupation, body areas satisfaction, and subjective evaluation was reported 0.87, 0.85, 0.82, 0.79, and 0.75, respectively. The reliability of this questionnaire the subscales of appearance evaluation, appearance orientation, fitness evaluation, fitness orientation, health evaluation, health orientation, illness orientation, physical satisfaction, subjective weight, weight preoccupation, and total score of the questionnaire was obtained α=0.74, α=0.79, α=0.85, α=0.81, α=0.74, α=0.86, α=0.81, α=0.80, α=0.79, α=0.77, and α=0.77, respectively.
-Shame questionnaire was developed by Cook [47]. This questionnaire consists of 30 questions and two subscales of shyness with 24 items (1, 2, 3, 4, 5, 6, 7, 9, 10, 11, 12, 15, 16, 17, 18, 20, 21, 22, 23, 24, 25, 27, 28, 30) and self-esteem with 6 items (8, 13, 14, 19, 26, 29). Questions are answered based on a 5-point Likert scale (Never: 0; Always: 4). The possible score range is 0 and 120. A high score indicates worthlessness, incompetence, and feelings of inferiority, emptiness, and loneliness. However, a low score indicates high self-confidence. Cook reported the Cronbach's alpha reliability coefficient of the shyness and low self-esteem subscales as 0.94 and 0.90, respectively. This researcher stated that the content validity of this questionnaire is acceptable (CVI=0.88) [47]. In a study by Rajabi & Abbasi [48], Cronbach's alpha reliability coefficients of the Shame Questionnaire were reported 0.90 for the whole sample, 0.89 for men, and 0.91 for women. In the present study, the reliability of subscales of shyness and low self-esteem and the total score of the questionnaire was reported α=0.85, α=0.89, and α=0.87, respectively.
The study was approved by the Ethics Committee of Aja University of Medical Sciences. The questioners took the questionnaires to any place selected by the participants (home, workplace, or any other place). The purpose of this study was explained to the participants, and their consent to participate in this study was considered, and they were allowed to
leave it at any stage of the process they wanted. In a private space, they were asked to complete the questionnaires and give them to the questioners. Due to the covid-19 conditions and the ease of work of participants, the online questionnaire option was also offered to them; thus, 48 questionnaires were filled in online.
Correlational structural equation modeling -a combination of path analysis and confirmatory factor analysis- was used. Pearson correlation matrix, multiple regression, and path analysis were used to analyze inferential statistics and frequency, the mean and standard deviation for descriptive statistics, and hypothesis testing. Data were analyzed by SPSS 25 and Amos 23.
Findings
Finally 195 questionnaires were analyzed. Demographic findings showed in Table 1.
Results of body image, shame, and attachment style among veteran amputees were showed in Table 2.
The results indicate an acceptable fit of the proposed model (Table 3). The general model proposed had a good fit. The g path coefficients were significant in all paths (p<0.05). Also, all β coefficients of shame attachment styles were significant (p<0.05). This means that the assumed direct causal paths of the general pattern were well-validated, and its indirect paths were confirmed (Figure 1).
Table 1) Demographic findings of participants in the research sample group (N=195)
Table 2) Descriptive findings of body image, shame, and attachment style among veteran amputees
Table 3) Fit indices of the proposed model
Figure 1) The final structural pattern of shame-based model based on body image mediated by attachment styles among veteran amputees
Discussion
The present study aimed to present a structural model and investigate body image and shame mediated by adult attachment among veteran amputees. The results of testing and estimating the structural model showed that the body image-based shame mediated by adult attachment has a good fit among veteran amputees. The results of the Pearson correlation coefficient showed that the correlation between secure, avoidant and anxious attachment styles with body image among veteran amputees was 0.398, -0.396 and -0.283, respectively. The regression analysis results also showed that predictor variables (secure, avoidant and anxious attachment styles) were able to significantly predict the criterion variable (body image of veteran amputees). The coefficient of determination of the model also shows that the predictor variables (secure, avoidant and anxious attachment styles) have explained 19.5% of the changes in the body image component of veteran amputees. Also, the Pearson correlation coefficient results showed that the shyness and low self-esteem components (as subscales of shame) had -0.445 and -0.227 correlation with secure attachment style, 0.504 and 0.267 with avoidant attachment style and 0.435 and 0.16 with anxious attachment style among veteran amputees, respectively. Also, the regression analysis results showed that the predictor variables (shyness and low self-esteem) were able to significantly predict the criterion variable (secure attachment style of veteran amputees). The coefficient of determination of the model also shows that the predictor variables (shyness and low self-esteem) have explained the changes in the attachment style among veteran amputees. Finally, the correlation coefficient results showed that the shyness and low self-esteem components had a negative correlation with body image among veteran amputees (had 0.447 and -0.315, respectively. Also, the regression analysis results showed that the predictor variables (shyness and low self-esteem) were able to significantly predict the criterion variable (body image of veteran amputees). The determination coefficient of the model also shows that the predictor variables (shyness and low self-esteem) were able to explain 21.3% of the changes in the body image component of veteran amputees.
The present study results on the relationship between body image and explaining the variance of attachment styles of veteran amputees were consistent with research [49-54]. These studies showed that the higher the body image satisfaction, the higher the score of secure attachment, and the less satisfied a person is with his/her body image, the higher his/her insecure attachment score will be. To explain this result, it can be stated that body image is the belief and perception human beings have about their physical condition. In other words, the body image contains ideas, conscious and unconscious feelings about the body [51]; Thus, a negative mental image of oneself can lead to dissatisfaction with the body, feeling unattractive, and finally, mental preoccupation with the appearance of a part of the body, even to the point of dysfunction. Therefore, a negative body image can affect veterans' cognitive and emotional processing styles, disrupting their mental order. This process can damage the process and the cycle of attachment by disrupting veterans' cognitive, psychological, and emotional performance [54].
On the other hand, people's internal function model can remain constant for many years, and people with avoidant and ambivalent attachment styles react to themselves and others based on their initial expectations. These people are expected to be constantly worried and anxious about their characteristics and the possibility of others' critical evaluations due to the feeling of insecurity in dealing with their daily affairs, interpersonal relationships, and negative self-image. A person's body image is also affected by this pervasive anxiety because it is part of their obvious aspects. In support of this claim, Vernon Davis shows that insecure attachment, especially ambivalent attachment, is positively associated with cosmetic surgery [53]. Insecure attachment leads to intense seeking the approval of others and worrying about gaining or maintaining the love of important people in life. These concerns lead to the use of various methods to maintain positive attention, including cosmetic surgery in order to enhance physical beauty. Therefore, body image anxiety can be part of a person's overall concern for themselves and arises from the internal function model (I am not lovable) [53].
The present study results on the relationship between attachment styles and the shame of veteran amputees and explaining the variance of this variable are consistent with research [22, 55, 56]. To explain this finding, it can be said that attachment is a kind of active internal model that is influenced by the family environment of the individual from early childhood and is often formed as a result of wrong upbringing during childhood [57]. In this regard, Bowlby [58] does not explicitly focus on shame. However, his theory largely refers to the relationship between shame and attachment, where he suggests that his internal function model complement the attachment styles and a child whose parents treat them as the unwanted person may, in addition to receiving a sense of unwontedness from their parents, believes that they are inherently unwanted and that everyone else in their mind will label them as an unwanted person [59]. In this regard, people with disabilities are likely to have this label of being unwanted in society in their minds because they are not as efficient as healthy people (Although this is probably not the case, and they are considered national heroes). Overall, positive and negative self-attention, which plays an important role in forming secure and insecure anxious attachment, explains painful self-blame and worthlessness in people with feelings of shame [60]. It seems that since people with secure attachment have a positive view of themselves and others and are less anxious, it makes sense to say that they have fewer problems and blame themselves less frequently; however, considering the inner characteristics of people with anxious attachment and a person prone to unhealthy shame, it can be said that when people have a negative view of themselves and a positive view of others, they try to keep others satisfied and establish constant communication; consequently, the subsequent anxiety increases their dependence on others and as a result, blames themselves under critical situations and constantly blames themselves. It also seems that a sense of shame, guilt, and self-punishment is created under such circumstances, making one more dependent on others. This is very likely among veteran amputees due to their special physical conditions.
On the other hand, it can be stated that shame attacks the core of veteran amputees' identity and is accompanied by feelings of diminution, worthlessness and helplessness [22]; therefore, the outcome of shame is the disruption of a person's mental and psychological order, which can even lead to the damage of their attachment. In addition, shame can affect self-esteem, sociability, and self-care or seeking care [55]. Shame arises from the difference between self and self-ideal. According to research [56], people prone to shame are more likely to experience psychological and interpersonal problems. This also confirms the vulnerability of mental health, emotional health and attachment of people to the incidence of shame. In another explanation, it can be said that one of the important components of shame is self-evaluation and self-criticism. Therefore, it seems that shame can easily make people think about self-critical styles and thus leads to increased vulnerability to a wide range of problems, such as damage to their attachment cycle.
Regarding the relationship between the dimensions of shame (shyness and low self-esteem) with body image among veteran amputees as another research finding, it can be said that this finding is consistent with researches [16-21]. For example, in a study of the role of body image in the emergence of shame, Ferreira et al. [21] found that people who have a more distorted self-body description perceive more shame. However, people who are not sensitive to their body image also perceive less shame. To explain this finding, it can be stated that the perception of a long-distance between the real bodily self and the ideal bodily self, especially among veterans, does not in itself affect their quality of life, but it seems that this perception somehow puts the individual in a passive situation, which creates a sense of shame in them [16]. This passive situation causes these people to engage in mental occupations about physical defects, obsessive behaviors such as physical examination and monitoring, cosmetic surgeries of the injured organ, and shame. It can be said that shame is both the cause and the result of this situation among obese and overweight people [20].
On the other hand, considering the current finding on the relationship between shyness and low self-esteem with body image among veteran amputees, it should be said that shy people are afraid of negative evaluation. Shyness is a complex mental, psychological, and social phenomenon characterized by anxiety in social situations, social inhibitions, or interpersonal behaviors resulting from concerns about interpersonal evaluation. People who are shy and do not have high self-esteem have less mental health and psychological stubbornness than extrovert people. Therefore, shyness causes people to feel internally weak and have a vulnerable body image due to low self-confidence in the face of external problems such as amputation. On the other hand, the results showed that self-esteem is also related to body image. Self-esteem is defined as the evaluation (emotional or logical) of a person of his or her relatively stable set of (positive or negative) beliefs about his or her specific traits, abilities, and friendships with others. Therefore, self-esteem is a value that contains self-concept internal information for a person and leads to the formation of self-esteem, sense of worth and self-confidence, and self-competency [16]. Accordingly, self-esteem is an aspect of self-concept that arises from one's judgments about one's worth and the feelings associated with those judgments. People with high self-esteem are flexible in the face of potentially challenging issues and are more likely to engage in identity exploration and not feel an inner gap. However, low self-esteem causes veteran amputees to feel weak due to their physical conditions and, as a result, perceive a weak body image.
Like any other study, the present study has some limitations, such as the limitation of the sample to veteran amputees. Also, the study population included veteran amputees in Tehran, so caution must b exercised while generalizing the results of this study to other people with disabilities and other cities. Lack of identification and control of variables affecting shame, body image and attachment of veteran amputees was another limitation of the present study. Because influential factors may be involved in the research results, it can also be pointed out that random sampling methods are not used due to the specific sensitivities of the study population. Considering the mentioned limitations, it is suggested that the present study, in addition to the veteran amputees, be performed on other disabled groups and other cities with different subcultures to ensure higher generalizability. It is also suggested to identify environmental, family and social factors affecting the feelings of shame, body image and attachment among veteran amputees in a future qualitative study and separate their effect from independent variables. Finally, it is suggested to use random sampling methods to increase the external validity of the research.
Conclusion
The mediating role of secure and avoidant attachment styles between body image and the shame of veteran amputees was confirmed. Finally, the findings indicated a good fit of the proposed model.
Acknowledgments: Thanks to everyone who helped us with this research.
Ethical Permissions: The study protocol was approved by the Ethics Committee of Aja University of Medical Sciences (IR.AJAUMS.REC.1398.105).
Conflicts of Interests: The authors declare no conflict of interest.
Authors’ Contribution: Yousefi N. (First Author), Introduction writer/Original researcher/Statistical analyst (40%); Tofangchiha Sh. (Second Author), Discussion writer (35%); Rahnejat A.M. (Third Author), Methodologist (25%).
Funding/Support: The authors receive no financial support for this research.
Keywords:
References
1. Shayanmehr A. Sociology of War. Tehran: Sociologists Publications; 2012. [Persian] [Link]
2. Anbari M, Oveisi Fardoei G. Cultural and identity challenges of Janbazan in the imposed war. Soc Rev. 2013;19(2):113-40. [Persian] [Link]
3. Shariati Mazinani S, Foroughzadeh S. Social challenges and life problems of veterans (case study: Veterans under 25% in Khorasan Razavi province. Q J Soc Dev. 2019;14(1):95-126. [Persian] [Link]
4. Gallagher P, Maclachlan M. Adjustment to an artificial limb: A qualitative perspective. J Health Psychol. 2001;6(1):85-100. [Link] [DOI:10.1177/135910530100600107]
5. Sarvestani AS, Azam AT. Amputation: A ten-year survey. Trauma Mon. 2013;18(3):126-9. [Link] [DOI:10.5812/traumamon.11693]
6. Resnik L, Ekerholm S, Borgia M, Clark MA. A national study of Veterans with major upper limb amputation: Survey methods, participants, and summary findings. Plos One. 2019;14(3):0213578. [Link] [DOI:10.1371/journal.pone.0213578]
7. Keeling M, Williamson H, Williams V, KIff J, Harcourt D. Body image concerns and psychological well-being among injured combat veterans with scars and limb loss: A review of the literature. Mil Behav Health. 2021;9(1):1-10. [Link] [DOI:10.1080/21635781.2020.1792013]
8. Cash T. Encyclopedia of body image and human appearance. Philadelphia: Elsevier; 2012. [Link]
9. Breakey JW. Body image: The lower-limb amputee. J Prosthet Orthot. 1997;9(2):58-66. [Link] [DOI:10.1097/00008526-199704000-00004]
10. Bessell A, Dures E, Semple C, Jackson S. Addressing appearance-related distress across clinical conditions. Br J Nurs. 2012;21(19):1138-43. [Link] [DOI:10.12968/bjon.2012.21.19.1138]
11. Bowers B. Providing effective support for patients facing disfiguring surgery. Br J Nurs. 2008;17(2):94-8. [Link] [DOI:10.12968/bjon.2008.17.2.28135]
12. Murray CD. Being like everybody else: The personal meanings of being a prosthesis user. Disabil Rehabil. 2009;31(7):573-81. [Link] [DOI:10.1080/09638280802240290]
13. Jayarajah U, Samarasekera DN. Psychological adaptation to alteration of body image among stoma patients: a descriptive study. Indian J Psychol Med. 2017;39(1):63-81. [Link] [DOI:10.4103/0253-7176.198944]
14. Desrochers J, Frengopoulos C, Payne MW, Viana R, Hunter SW. Relationship between body image and physical functioning following rehabilitation for lower-limb amputation. Int J Rehabil Res. 2019;42(1):85-8. [Link] [DOI:10.1097/MRR.0000000000000329]
15. Lamarche L, Ozimok B, Gammage KL, Muir C. Men respond too: The effects of a social-evaluative body image threat on shame and cortisol in university men. Am J Mens Health. 2017;11(6):1791-803. [Link] [DOI:10.1177/1557988317723406]
16. Duarte C, Pinto‐Gouveia J, Ferreira C, Batista D. Body image as a source of shame: A new measure for the assessment of the multifaceted nature of body image shame. Clin Psychol Psychother. 2015;22(6):656-66. [Link] [DOI:10.1002/cpp.1925]
17. Ferreira C, Pinto-Gouveia J, Duarte C. Self-compassion in the face of shame and body image dissatisfaction: Implications for eating disorders. Eat Behav. 2013;14(2):207-10. [Link] [DOI:10.1016/j.eatbeh.2013.01.005]
18. Mendes AL, Canavarro MC, Ferreira C. How psychological inflexibility mediates the association between general feelings of shame with body image-related shame and eating psychopathology severity. Appetite. 2021;163:105228. [Link] [DOI:10.1016/j.appet.2021.105228]
19. Gioia F, Griffiths MD, Boursier V. Adolescents' body shame and social networking sites: The mediating effect of body image control in photos. Sex Roles. 2020;83(11):773-85. [Link] [DOI:10.1007/s11199-020-01142-0]
20. Duarte C, Pinto-Gouveia J. The impact of early shame memories in Binge Eating Disorder: The mediator effect of current body image shame and cognitive fusion. Psychiatry Res. 2017;258:511-7. [Link] [DOI:10.1016/j.psychres.2017.08.086]
21. Ferreira C, Dias B, Oliveira S. Behind women's body image-focused shame: Exploring the role of fears of compassion and self-criticism. Eat Behav. 2019;32:12-7. [Link] [DOI:10.1016/j.eatbeh.2018.11.002]
22. Brown J, Trevethan R. Shame, internalized homophobia, identity formation, attachment style, and the connection to relationship status in gay men. Am J Mens Health. 2010;4(3):267-76. [Link] [DOI:10.1177/1557988309342002]
23. Ellingsen T, Johannesson M, Tjotta S, Torsvik G. Testing guilt aversion. Games Econom Behav. 2010;68(1):95-107. [Link] [DOI:10.1016/j.geb.2009.04.021]
24. Arditte KA, Morabito DM, Shaw AM, Timpano KR. Interpersonal risk for suicide in social anxiety: The roles of shame and depression. Psychiatry Res. 2016;239:139-44. [Link] [DOI:10.1016/j.psychres.2016.03.017]
25. Budden A. The role of shame in post-traumatic stress disorder: A proposal for a socio-emotional model for DSM-V. Soc Sci Med. 2009;69(7):1032-9. [Link] [DOI:10.1016/j.socscimed.2009.07.032]
26. Szentagotai-Tatar A, Nechita DM, Miu AC. Shame in anxiety and obsessive-compulsive disorders. Curr Psychiatry Rep. 2020;22(4):1-9. [Link] [DOI:10.1007/s11920-020-1142-9]
27. Lund P. Christian faith and recovery from substance abuse, guilt, and shame. J Relig Spiritual Soc Work Soc Thought. 2017;36(3):346-66. [Link] [DOI:10.1080/15426432.2017.1302865]
28. Cella S, Iannaccone M, Cotrufo P. Does body shame mediate the relationship between parental bonding, self-esteem, maladaptive perfectionism, body mass index and eating disorders? a structural equation model. Eat Weight Disord. 2020;25(3):667-78. [Link] [DOI:10.1007/s40519-019-00670-3]
29. Velotti P, Garofalo C, Bottazzi F, Caretti V. Faces of shame: Implications for self-esteem, emotion regulation, aggression, and well-being. J Psychol. 2017 Feb 17;151(2):171-84. [Link] [DOI:10.1080/00223980.2016.1248809]
30. Matos M, Pinto-Gouveia J, Gilbert P. The effect of shame and shame memories on paranoid ideation and social anxiety. Clin Psychol Psychother. 2013;20(4):334-349. [Link] [DOI:10.1002/cpp.1766]
31. Gambin M, Sharp C. The relations between empathy, guilt, shame and depression in inpatient adolescents. J Affect Disord. 2018;241:381-7. [Link] [DOI:10.1016/j.jad.2018.08.068]
32. Bannister JA, Colvonen PJ, Angkaw AC, Norman SB. Differential relationships of guilt and shame on post-traumatic stress disorder among veterans. Psychol Trauma. 2019;11(1):35-42. [Link] [DOI:10.1037/tra0000392]
33. Swiger T. Morally injurious experiences of combat exposed veterans of Iraq and Afghanistan: Moderating effects of self-forgiveness on feelings of shame and guilt [dissertation]. Morgantown: West Virginia University; 2020. [Link]
34. Cunningham KC, LoSavio ST, Dennis PA, Farmer C, Clancy CP, Hertzberg MA, et al. shame as a mediator between post-traumatic stress disorder symptoms and suicidal ideation among veterans. J Affect Disord. 2019;243:216-9. [Link] [DOI:10.1016/j.jad.2018.09.040]
35. Kerr ML, Rasmussen HF, Smiley PA, Fanning KA, Buttitta KV, Benson L, et al. Within-and between-family differences in mothers' guilt and shame: Caregiving, coparenting, and attachment. J Fam Psychol. 2021;35(3):265-75. [Link] [DOI:10.1037/fam0000647]
36. McWilliams LA, Bailey SJ. Associations between adult attachment ratings and health conditions: Evidence from the national comorbidity survey replication. Health Psychol. 2010;29(4):446-53. [Link] [DOI:10.1037/a0020061]
37. Holmes J. John Bowlby and attachment theory. Abingdon: Routledge; 2014. [Link] [DOI:10.4324/9781315879772]
38. Schore AN. All our sons: The developmental neurobiology and neuroendocrinology of boys at risk. Infant Ment Health J. 2017;38(1):15-52. [Link] [DOI:10.1002/imhj.21616]
39. Canavarro MC, Dias P, Lima V. Avaliacao of the adult link: A review or criticism of the application of the adult attachment scale-R (ASS-R) to the Portuguese population. Psicologia. 2006;20(1):156-86. [Spanish] [Link] [DOI:10.17575/rpsicol.v20i1.381]
40. Granqvist P. Attachment, culture, and gene-culture co-evolution: Expanding the evolutionary toolbox of attachment theory. Attach Hum Dev. 2021;23(1):90-113. [Link] [DOI:10.1080/14616734.2019.1709086]
41. Aikins JW, Howes C, Hamilton C. Attachment stability and the emergence of unresolved representations during adolescence. Attach Hum Dev. 2009;11(5):491-512. [Link] [DOI:10.1080/14616730903017019]
42. Collins NL, Read SJ. Adult attachment, working models, and relationship quality in dating couples. J Pers Soc Psychol. 1990;58(4):644-63. [Link] [DOI:10.1037/0022-3514.58.4.644]
43. Tavakolizadeh J, Tabari J, Akbari A. Academic self-efficacy: predictive role of attachment styles and meta-cognitive skills. Procedia Soc behav sci. 2015;171:113-20. [Link] [DOI:10.1016/j.sbspro.2015.01.096]
44. Rezaei H, Hasani J, Noor Mohamadi Najafabadi M. The role of attachment in risky behaviors of male high school adolescent students. Knowl Res Appl Psychol. 2019;20(1):112-21. [Persian] [Link]
45. Brown TA, Cash TF, Mikulka PJ. Attitudinal body-image assessment: Factor analysis of the body-self relations questionnaire. J Pers Assess. 1990;55(1-2):135-44. [Link] [DOI:10.1080/00223891.1990.9674053]
46. Zarshenas S, Karbala'i Nouri A, Hosseini SA, Rahgozar M, Sayed Noor R, Moshtagh N. The effect of aerobic exercise on women's attitudes about body image. Arch Rehabil. 2010;11(2):15-20. [Persian] [Link]
47. Cook DR. Internalized shame scale: Technical manual. Toronto: Multi Health System; 2001. [Link]
48. Rajabi G, Abbasi G. The relationship between social anxiety and fear of failure with internalized shame in students. J Res Clin Psychol Couns. 2012;1(2):171-82. [Persian] [Link]
49. Barnes MA, Caltabiano ML. The interrelationship between orthorexia nervosa, perfectionism, body image and attachment style. Eat Weight Disord. 2017;22(1):177-84. [Link] [DOI:10.1007/s40519-016-0280-x]
50. Cash TF, Theriault J, Annis NM. Body image in an interpersonal context: Adult attachment, fear of intimacy and social anxiety. J Soc Clin Psychol. 2004;23(1):89-103. [Link] [DOI:10.1521/jscp.23.1.89.26987]
51. Lev‐Ari L, Baumgarten‐Katz I, Zohar AH. Show me your friends, and I shall show you who you are: The way attachment and social comparisons influence body dissatisfaction. Eur Eat Disord Rev. 2014;22(6):463-9. [Link] [DOI:10.1002/erv.2325]
52. Bex JM. An examination of the relationship between attachment style and body image in adolescent girls: A focus on the mother-daughter relationship [dissertation]. New York: Syracuse University; 2014. [Link]
53. Davis D, Vernon ML. Sculpting the body beautiful: Attachment style, neuroticism, and use of cosmetic surgeries. Sex Roles. 2002;47(3):129-38. [Link] [DOI:10.1023/A:1021043021624]
54. Orzolek-Kronner C. The effect of attachment theory in the development of eating disorders: Can symptoms be proximity-seeking. Child Adolesc Soc Work J. 2002;19(6):421-35. [Link] [DOI:10.1023/A:1021141612634]
55. Wells GB. Lesbians in psychotherapy: Relationship of shame and attachment style. J Psychol Hum Sex. 2004;15(2-3):101-16. [Link] [DOI:10.1300/J056v15n02_06]
56. Akbag M, Imamoglu SE. The prediction of gender and attachment styles on shame, guilt, and loneliness. Kuram Uygulamada Egitim Bilimleri. 2010;10(2):669-82. [Link]
57. Clifford CE. Attachment and covert relational aggression in marriage with shame as a potential moderating variable: A two wave panel study [dissertation]. Provo: Brigham Young University; 2013. [Link]
58. Bowlby EJM. Separation, anxiety and anger: Attachment and loss volume 2. New York: Random House; 2010. [Link]
59. Besser A, Priel B. Models of attachment, confirmation of positive affective expectations, and satisfaction with vacation activities: A pre-post panel design study of leisure. Pers Individ Differ. 2006;41(6):1055-65. [Link] [DOI:10.1016/j.paid.2006.04.011]
60. Mallinckrodt B, Wei M. Attachment, social competencies, social support, and psychological distress. J Couns Psychol. 2005;52(3):358-67. [Link] [DOI:10.1037/0022-0167.52.3.358]
Send email to the article author